
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
1
RECORDS MANAGEMENT
CODE OF PRACTICE FOR
HEALTH AND SOCIAL
CARE 2022
A GUIDE TO THE MANAGEMENT
OFHEALTH AND CARE RECORDS
gov.wes
PUBLISHED FEBRUARY 2022
2
Contents
Introduction
Section 1: Scope of the code
Section 2: Records management obligations
Section 3: Organising records
Section 4: Records storage for operational use
Section 5: Management of records when the minimum retention period is reached
Appendix I: Public and statutory inquiries
Appendix II: Retention schedule
Appendix III: How to deal with specific types of records
Appendix IV: Records at contract change
1
3
5
10
15
19
28
29
60
77
© Crown copyright 2022 WG44221 Digital ISBN 978-1-80391-679-8
Mae’r ddogfen yma hefyd ar gael yn Gymraeg.
This document is also available in Welsh.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
1
Introduction
The Records Management Code of Practice for Health and Social Care2022 (from this point onwards
referred to as the Code) is a guide for you to use in relation to the practice of managing records.
Itis relevant to organisations working within, or under contract to, the NHS in Wales. The Code also
applies to adult social care and public health functions commissioned or delivered by local authorities.
The Code is based on the Records Management Code of Practice for Health and Social Care 2021
developed by NHSX in England, and provides a framework for consistent and eective records
management based on established standards and current legislation. It includes guidelines on topics
such as legal, professional, organisational and individual responsibilities when managing records. It also
advises on how to design and implement a records management system including advice on organising,
storing, retaining and deleting records. It applies to all records regardless of the media they are held on.
Whereverpossible organisations should be moving away from paper towards digital records.
The Code is accompanied by a number of important appendices:
• Appendix I refers to information on public inquiries.
• Appendix II is a retention schedule for dierent types of records.
• Appendix III is detailed advice on managing dierent types and formats of records such as integrated
care records and sta records.
All organisations and managers need to enable sta to conform to the standards in this Code.
Thisincludes identifying organisational changes or other requirements needed to meet the standards,
for example, the people, money and correct tools required. Information governance performance
assessments, such as the Wales Information Governance Toolkit hosted by Digital Health and Care
Wales (DHCW), and your own organisation management arrangements will help you identify any
necessary changes to your current records management practices. Thosewho have responsibilities for
monitoring overall performance, like NHS organisations in Wales, Healthcare Inspectorate Wales (HIW),
Audit Wales and the Information Commissioner’s Oce (ICO) help ensure eective management systems
are in place. An example is by inspecting sites as part of their key lines of enquiry and statutory powers.
The guidelines in this Code published by NHSX in England drew on published guidance from
TheNational Archives (TNA) and best practice andlessons learnt in the public and private sectors.
This Code must also be read in conjunction with the following:
• Professional Records Standards Body (PRSB) structure and content ofhealth and care records
standards.
• Academy of Medical Royal Colleges’ standards for the clinical structure and content of patient records.
• Code of Practice on the management of records issued under Section 46 of the Freedom of
Information Act 2000 (FOIA) 2000.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
2
This 2022 revision was conducted by Health and Social Services’ Digital Policy Team, based on NHSX
guidance, reflecting consultations in which 50 organisations responded, including national stakeholders
and local organisations. This Code replaces the previous guidance:
• WHC 2000 (71): For the record – Managing Records in NHS Trusts and Health Authorities.
Equit
This Code of Practice has been subject to an equality assessment. Following assessment, thispolicy
was not felt to be discriminatory or detrimental in any way with regard to the protected characteristics,
theWelsh Language or carers.
Review
The Code of Practice will be in place for 1 year before a review, unless legislation changes in which case it
will be updated as appropriate. Following this, it is recommended that the code isreviewed every 5 years.
Standards and practice covered by the Code will change over time so this document will be updated
as necessary. In particular, it should be noted that at the time of writing there are a number of on-going
public inquiries including the Independent Inquiry into Historic Child Sex Abuse (IICSA) and Infected Blood
Public Inquiry (IBI). This means that records must not be destroyed until guidance is issued by the inquiry.
Futureinquiries may lead to further specific records management requirements being set. Where that
happens, the Inquiry will publish additional guidance on its website.
It should also be noted a review into the retention time for de-registered GP records is being conducted.
De-registered refers to when a patient is no longer on the GP practice system. Itdoes not refer to patients
who are still registered at a GP practice but have not needed to receive care. If a patient has moved to
another practice, the record would be sent to the new provider. However, if the reason for de-registration
is unknown, a copy is sent to Primary Care Services inNHS Wales Shared Service Partnership. We are
proposing to review the retention time for de-registered GP records to ensure that the significant costs
of retaining the records for 100 years are justified by the benefits they bring. We will look, for example,
athow many records are recalled and what the reasons are.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
3
Section 1:
Scope of the code
1.1 Overview
This section explains the legal definition of
arecord and the types of records in scope of
theCode.
1.2 Wht is record?
There are a couple of definitions of a record,
which are useful to highlight. The ISO standard
ISO 15489-1:2016 defines a record as:
“Information created, received, and maintained
asevidence and as an asset by an organisation
orperson, in pursuance of legal obligations or
inthe transaction of business.”
Section 205 of the Data Protection Act 2018
defines a health record as a record which:
• consists of data concerning health,
• has been made by or on behalf of a health
professional in connection with the diagnosis,
care or treatment of the individual to whom
thedata relates.
1.3 Scope of records covered
bthe code
The guidelines in this code apply to NHS and
adult social care records in Wales.
This includes:
• records of Welsh patients treated by
NHSorganisations in England or Wales;
• records of patients treated on behalf of
NHSWales in the private healthcare sector;
• records of private patients treated on NHS
Wales premises;
• records created by providers contracted to
deliver NHS services in Wales (for example,
GPservices);
• adult service user records who receive social
care support;
• jointly held records;
• records held as part of a shared care records
programme;
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
4
• records held by local authorities such as public
health records, contraceptive and sexual health
service records;
• sta records;
• complaints records;
• corporate records – administrative records
relating to all functions of the organisation.
The Code does not cover children’s social care
records. These are within the remit of Local
Authorities.
Whilst not strictly covered by this guide,
privateproviders can also use this Code for
guidance in relation to their records management.
ThePrivate and Voluntary Health Care (Wales)
Regulations2002 provide a legal framework
forprivate providers to manage their records.
There are a number of smaller health and care
providers that this Code will apply to, for example,
dental practices or independent care providers
providing an element of NHS or nursing care.
For some aspects of this Code, these small
organisations should take a pragmatic approach
to, for example, the application of security
classifications.
1.4 Tpe of records covered
bthe code
The guidelines apply regardless of the media
on which the records are held. Usually these
records will be on paper or digital. However,
somespecialties will include physical records,
such as physical moulds made from plaster of
Paris, referto Appendix III.
Examples of records that should be managed
using the guidelines in this Code include:
• health and care records;
• registers – for example, birth, death, Accident
and Emergency, theatre, minor operations;
• administrative records, for example, personnel,
estates, financial and accounting records,
notesassociated with complaint-handling;
• X-ray and imaging reports, output and images;
• secondary uses records (such as records
that relate to uses beyond individual care),
for example, records used for service
management, planning, research.
Examples of record formats that should be
managed using the guidelines from this code:
• digital;
• paper;
• photographs, slides, and other images;
• microform (microfiche or microfilm);
• physical records (records made of physical
material such as plaster, gypsum and
alginatemoulds);
• audio and video tapes, cassettes, CD-ROM etc;
• emails;
• computerised records;
• scanned records;
• text messages (SMS) and social media
(both outgoing from the NHS and incoming
responses from the patient or service user)
such as Twitter and Skype;
• metadata added to, or automatically created
by, digital systems when in use – content
can sometimes be of little value if it is not
accompanied by relevant metadata;
• websites and intranet sites that provide
key information to patients or service users
andsta.
Appendix III provides further details about
managing specific types of records, for example,
complaints records.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
5
Section 2:
Records mngement
obigtions
2.1 Overview
All health and care employees are responsible
formanaging records appropriately.
Recordsmust be managed in accordance with
the law. Healthand care professionals also
have professional responsibilities, for example,
followingthe Caldicott Principles records
keeping standards such as UK GDPR and
associated legislation, the Common Law Duty
of Confidentiality and other standards set out
by registrant bodies. Whilstevery employee
has individual responsibilities, each organisation
should have a designated member of sta who
leads on records management. Each organisation
should also have a policy statement on records
management which is made available to sta
through induction and training. Organisationsmay
be asked for evidence to demonstrate they
operate a satisfactory records management
regime.
2.2 Leg obigtions
Public Records Act 1958 and Local
Government Act 1972
The Public Records Act 1958 is the principal
legislation relating to public records. Recordsof
NHS organisations are public records in
accordance with Schedule 1 of the Act.
Thismeans that employees are responsible for
any records that they create or use in the course
of their duties. This includes records controlled
by NHS organisations under contractual or
other joint arrangements, or as inherited legacy
records of defunct NHS organisations. The Act
applies regardless of the format of the records.
TheMinister for Health and Social Services and
all NHS organisations in Wales have a duty under
the Act to make arrangements for the safekeeping
and eventual disposal of all types of records.
Thisincludes a list of some of the bodies deemed
to be public records bodies.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
6
Thisis carried out under the overall guidance and
supervision of the Keeper of Public Records who
reports annually on this to the Secretary of State
for Culture, Media and Sport who is accountable
toparliament. Further guidance on the definition
of Welsh public records bodies can be found in
the Government of Wales Act 2006, Section 148.
Public health and social care records, where a
local authority is the provider (or the provider is
contracted to provide services to a local authority),
must be managed in accordance with the
requirement to make proper arrangements under
Section 224 of the Local Government Act 1972.
This states that proper arrangements must be in
place with respect to any documents that belong
to or are in the custody of the council or any of
their ocers.
Where health and social care records are created
as a joint record or part of a system where local
health and care organisations can see the records
of other local health and care organisations,
thenthese records would be managed in line with
the requirements of the Public Records Act 1958
where one or more of the bodies that created the
joint record is a public record body.
The NHS Wales Standard Contract 2006 notes
acontractual requirement on organisations
which are not bound by either the Public Records
Act1958 or the Local Government Act 1972 to
manage the records they create. Thereare also
statutory requirements aecting both private
and voluntary care providers as set out in the
Private and Voluntary Health Care (Wales)
Regulations2002.
Freedom of Information Act 2000
The Freedom of Information Act (FOIA) governs
access to and management of non-personal
public records. The FOIA was designed to
create transparency in government and allow
any citizen to know about the provision of public
services through the right to submit a request for
information.
This right is only as good as the ability of those
organisations to supply information through good
records management programmes. Records
managers should adhere to the Code of Practice
on Record Keeping issued by the Secretary
of State for Culture, Mediaand Sport, under
Section46 of the FOIA. Thesection46 Code
of Practice is used as a statutory statement of
good practice by the regulator and the courts.
TheInformation Commissioner regulates
compliance with FOIA, and provides detailed
guidance on the ICO’swebsite.
UK GDPR and Data Protection Act 2018
The UK GDPR is the principal legislation governing
how records, information and personal data are
managed. It sets in law how personal and special
categories of information may be processed.
TheData Protection Act 2018 principles are also
relevant to the management of records. Underthe
UK GDPR, organisations may be required to
undertake Data Protection Impact Assessments
(DPIA) as set out in Section 3 of this Records
Management Code.
The UK GDPR also introduces a principle of
accountability. The Information Commissioner’s
Oce (ICO) Accountability Framework can
support organisations with their obligations.
Goodrecords management will help organisations
to demonstrate compliance with this principle.
TheInformation Commissioner regulates
compliance with UK GDPR and related legislation.
Detailed guidance on all aspects of data
protection is available at www.ico.org.uk.
Health and Social Care Act 2008
Regulation 17 under the Health and Social Care
Act 2008 requires that health and care providers
must securely maintain accurate, complete and
detailed records for patients or service users,
employment of sta and overall management.
HIW are responsible for regulating this and HIW
may have regard to the Code when assessing
providers’ compliance with this regulation.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
7
The Welsh Language (Wales) Measure 2011
Legislation and policy in Wales support the
Welsh language recording on patient and clinical
records. The Welsh Language Measure gives the
Welsh language ocial status in Wales and the
requirement to actively oer services in Welsh
is a key principle of the More than just words
framework.
Further details on the protocol of which language
to record a consultation between a practitioner
and a service user can be found in AppendixIII
under ‘Welsh and English language record
guidance’.
Other relevant legislation
Other legislation requires information to be held
as proof of an activity against the eventuality
of a claim. Examples of legislation include the
Limitation Act 1980 or the Consumer Protection
Act 1987. The Limitation Act sets out the length of
time you can bring a legal case after an event and
sets it at six years. This forms the basis for some
ofthe retention periods set out in Appendix II.
2.3 Profession obigtions
Sta who are registered to a professional
body, such as the General Medical Council
(GMC), Nursing and Midwifery Council (NMC)
or Social Care Wales will be required to adhere
to record keeping standards defined by their
registrant body. This is designed to guard against
professional misconduct and to provide high
quality care in line with the requirements of
professional bodies.
The Academy of Medical Royal Colleges (AoMRC)
generic medical record keeping standards
were prepared for use in the NHS across the UK,
primarily in acute settings but the standards are
useful for all health and care settings. The AoMRC
notes that a medical record, whether paper or
digital, must adhere to certain record keeping
standards. The Royal College of Nursing has
produced guidance on abbreviations and other
short forms in patient or client records.
Further information about professional standards
for records can be obtained from your relevant
professional body. The main standard setting
bodies in health and social care in Wales are:
• Academy of Medical Royal Colleges;
• British Medical Association;
• General Medical Council;
• Health and Care Professions Council;
• Royal College of Midwives;
• Royal College of General Practitioners;
• Nursing and Midwifery Council;
• Social Care Wales.
There are also organisations that provide advice
specifically to records managers and archivists.
These are:
• The Federation for Informatics Professionals;
• The National Archives;
• The Archives and Records Association;
• The Institute of Health Records and
Information Management;
• Information and Records Management
Society.
Caldicott principles
The Caldicott principles outline eight areas that
health and social care sta should aim to follow
inaddition to the UK GDPR.
2.4 Mngement responsibiities
Records management should be recognised as
a specific corporate responsibility within every
organisation. It should provide a managerial focus
for records of all types, in all formats throughout
their lifecycle, from creation through to ultimate
disposal. The records management function
should have clear responsibilities and objectives
and be adequately resourced to achieve them.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
8
A designated member of sta of appropriate
seniority, ideally with suitable records
management qualifications, should have lead
responsibility for records management within
the organisation. This could be a care home
manager or practice manager or in a larger
organisation, a sta member reporting directly
to a board member. This lead role should be
formally acknowledged, included in relevant job
descriptions and communicated throughout the
organisation. It is essential that the managers
responsible for the records management
function is directly accountable to or works in
close association with the managers responsible
for other information governance work areas.
Whennew IT projects or upgrades are introduced,
the person responsible for Records Management
should be closely involved.
As records management activities are undertaken
throughout the organisation, mechanisms
must bein place to enable the designated
corporate lead to exercise an appropriate level
ofmanagement of this activity, even where there
is no direct reporting line. This might include
cross-departmental records and information
working groups or individual information and
records champions or coordinators who may
alsobe information asset owners.
Training
All sta, whether working with clinical or
administrative records, must be appropriately
trained so that they are competent to carry
out their designated duties and fully aware
of their personal responsibilities in respect
of record keeping and records management.
No patient/service users’ records or systems
should be handled or used until training has
beencompleted.
Training must include the use of electronic records
systems and it must be undertaken through
the generic and/or Health Board-wide training
programmes, which can be department orcontext
specific.
Health Boards with Information Governance
training should also include Records Management
in this training. Training should be complemented
by appropriate organisation policies, procedures
and guidance documentation.
All sta employed by the NHS in Wales
will receive information on their personal
responsibilities for record keeping in contracts
of employment. Thisincludes the creation, use,
storage, securityand confidentiality of health
records. Appropriate training will be given to
all health records sta on the systems used to
maintain records and these will meet local and
national standards. All new employees to NHS
organisations in Wales will be given basic records
practice training as part of the induction process.
Training to help identify records for
permanent preservation that should be send
to the Place of Deposit can be provided by
TheNationalArchives.
Professional standards of record keeping are
governed by the associated Royal colleges.
Thesestandards should form part of the
professional practice review.
2.5 Orgnistion poic
Each board, trust or organisation must have an
overall policy statement on how it manages all
ofits records. This may be a standalone policy or
part of the overall suite of IG policies. The policy
should include details of how the organisation will
use the records it creates. For example, as well
as records being used to plan and deliver care,
theywill also be used for service improvement
and research.
This statement must be endorsed by
the Operational Management Team,
board(orequivalent) and made available to all
sta at induction and through regular updates
andtraining.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
9
The policy statement should provide a mandate
for the performance of all records and information
management functions. In particular, it should set
out an organisational commitment to create, keep,
manage, and dispose of records and document
its principal activities in this respect. The policy
should also:
• outline the role of records management within
the organisation and its relationship to the
organisation’s overall strategy;
• define roles and responsibilities within the
organisation in relation to records, including the
responsibility of individuals to document their
actions and decisions – an example is, who is
responsible for the disposal of records;
• assign responsibility for the arrangements for
records appraisal, selection and transfer for the
permanent preservation of records (as required
by Section3 (1) of the Public Records Act 1958);
• provide a framework for supporting standards,
procedures and guidelines and regulatory
requirements (such as HIW and DHCW’s
IGtoolkit);
• indicate the way in which compliance with
the policy and its supporting standards,
procedures and guidelines will be monitored
and maintained;
• provide the mandate for final disposal of all
information by naming the committee or group
that oversees the processes and procedures;
• provide instruction on meeting the records
management requirements of the FOIA and
theUK GDPR.
The policy statement should be reviewed
at regular intervals (at least once every two
years) and if appropriate should be amended
to maintain its relevance. The policy is also
an important component of the organisation’s
information governance arrangements and should
be referenced in the organisation’s IG policies
orframework.
Organisations must also conduct an annual
survey to understand the extent of their records
management responsibilities and to help inform
future work-plans. It will aid organisations to know:
• what series of records it holds (and potential
quantities);
• the format of its records;
• the business area that created the record
(andpotential Information Asset Owner);
• disposal potential for the coming year.
Information Asset Management systems may
support this process. They can help identify
where records are held and whether they are
being held under the correct security conditions,
andin the case of health and care records,
remainconfidential. The process can also be used
as an opportunity for asset owners to identify how
long their records need to be held. The process
will identify business critical assets and ensure
that there are adequate business continuity
measures in place to assure access.
2.6 Monitoring records
mngement performnce
Organisations may be asked for evidence to
demonstrate they operate a satisfactory records
management regime. There is a range of
sanctions available if satisfactory arrangements
are not in place. Sanctions vary in their severity
for both organisations and the individual.
Theymayinclude:
• formal warning;
• professional de-registration: temporary
suspension or permanent;
• regulatory intervention: leading to conditions
being imposed upon an organisation,
ormonetary penalty issued by the ICO.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
10
Section 3:
Orgnising records
3.1 Overview
As set out in section two, each organisation must
have a policy for managing records. This section
describes how to design and implement a records
management scheme, decide what a record
is and arrange records. It includes information
about the importance of metadata and security
classifications.
3.2 Designing records
keepingsstem
A record keeping system should be implemented
at organisational level and within departmental
standard operating procedures as appropriate.
The records lifecycle, or the information lifecycle,
is a term that describes a controlled regime in
which information is managed from the point that
it is created to the point that it is either destroyed
or permanently preserved as being of historical
orresearch interest.
A records management system should cover each
stage of the lifecycle:
• creation: create and log quality information;
• using: use or handle;
• retention: keep or maintain in line with NHS
Wales’ recommended retention schedule;
• appraisal: determine whether records are
worthy of archival preservation;
• disposal: dispose appropriately according
topolicy.
Designing and Implementing Record Keeping
Systems (DIRKS) is a manual which led to the
creation of ISO 15489-1:2016 Information
and documentation – Records Management.
This standard, published by the International
Organization for Standardization (ISO), focuseson
the business principles behind records
management and how organisations can establish
a framework to enable a comprehensive records
management programme. The standard is an
eight-stage process and can be summarised as:
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
11
1. Conduct preliminary investigation.
2. Analyse business activity.
3. Identify requirements for records.
4. Assess existing systems.
5. Identify strategies to satisfy requirement.
6. Design records system.
7. Implement records systems.
8. Conduct post implementation review.
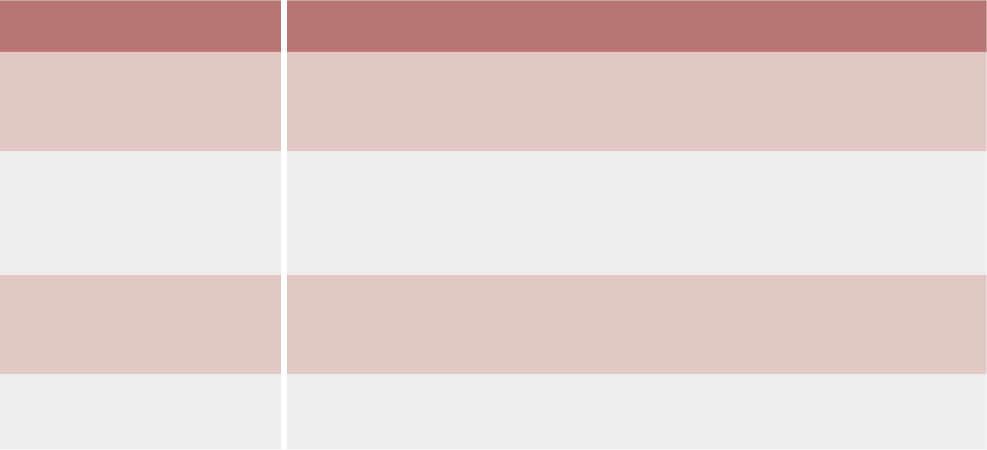
The standard also describes the characteristics
ofa record.
Record characteristic How to evidence
Authentic It is what it purports (claims) to be. To have been created or sent by the
person purported to have created or sent it. To have been created or
sent at the time purported.
Reliable Full and accurate record of the transaction or activity or fact.
Createdclose to the time of transaction or activity. Created by
individuals with direct knowledge of the facts or by instruments
routinely involved inthe transaction or activity.
Integrity Complete and unaltered. Protected against unauthorised alteration.
Alterations after creation can be identified as can the person making
thechanges.
Useable Located, retrieved, presented and interpreted. Context can be
established through links to other records in the transaction or activity.
These characteristics allow strategies, policies
and procedures to be established that will enable
records to be authentic, reliable, integral and
usable throughout their lifecycle.
In terms of ensuring a record is reliable, where an
organisation realises that inaccurate information
is being held about its patient or service users,
then it should take steps to rectify the situation
and make records as accurate as they can.
Anexample of what action might be taken can
be found in the Institute of Health Records and
Information Management (IHRIM) Good Practice
Guidance 2020.
There are a series of other British and international
standards that are used to produce record
keeping systems. These all interrelate and work
within the same guiding principles and where
possible use the same terminology. They all
rely upon defining roles and responsibilities,
processes, measurement, evaluation,
reviewandimprovement.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
12
3.3 Conducting Dt
Protection Impct Assessment
Under UK GDPR, organisations are required to
conduct Data Protection Impact Assessments
(DPIAs) where there is a new or change in use
of personal data and a potentially high risk to
privacy. (A DPIA template can be found on the
ICOwebsite). Some uses require a mandatory
DPIA (where processing is large scale or
introduces new technologies). If you are looking
to establish a new records management function,
then it will be vitally important to complete a DPIA.
This will highlight potential risks to privacy and
data protection, allowing you to action, mitigate or
eliminate that risk. This must be conducted prior
toany processing being carried out.
When you are looking to amend a record’s
function, you should check with the person
responsible for records management first, for
example, your record manager or your data
protection ocer. DPIA completion in this
circumstance will depend on the amendments you
are looking to make. For example, if you intend to
add three racking shelves for paper HR files to the
existing twenty shelves you would probably not
complete a DPIA. If you were looking to send your
records osite for scanning or destruction you
must complete a DPIA, as this is a new process
and the risk is greater.
If your DPIA identifies high risk that you cannot
mitigate, you must consult the ICO before starting
the processing.
3.4 Decring record
Within the record keeping system, there must be
amethod of deciding:
• what is a record;
• what needs to be kept;
• this process is described as “declaring a
record”. A record can be declared at the point
it is created or it can be declared at a later
date. The process of declaring a record must
be clear to sta. Adeclared record is then
managed in a way that will fix it in an accessible
format until it is appraised for further value or
disposed of, according to retention policy that
has been adopted. Some activities will be pre-
defined as creating a record that needs to be
kept, suchas health and care records or the
minutes and papers of board meetings. Other
records will need to fulfil the criteria as being
worth keeping, suchas unique instances of
a business document or email. Datasets may
also be declared as records andmanaged
accordingly.
Declared records can be held in the “businessas
usual” systems or they can be moved into a
protected area such as an Electronic Document
and Records Management System (EDRMS)
depending on the record keeping system in use.
Organisations’ teams should only hold the records
they need to conduct business locally.
Records and information relating to closed cases
may be kept locally for a short period of time (such
as a year). This is in case a patient or service user
re-presents or is re-referred. After that time, they
should be moved to long-term storage for the
rest of their retention period. For digital records,
a system may already be set up whereby records
no longer required for current business are stored
(such as a dedicated network drive or space on a
drive). Records should be moved there keeping
operational space free for current cases or work.
This will also restrict unnecessary access to non-
current personal or sensitive data.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
13
Your organisation’s records management policy
should cover what you need to do locally in
thiscircumstance.
Key legislation, such as the UK GDPR or FOIA,
applies to all recorded information of the types
covered by these Acts, whether declared as a
formal record or not. However, declaration makes
it easier to manage information in accordance with
the legislation and business needs. Requests for
information made under this legislation are easier
to find in a logical filing system. Accumulations
of informally recorded information, which can be
dicult to find, should therefore be minimised.
3.5 Orgnising records
Record keeping systems must have a means
of physically or digitally organising records.
Thisis often referred to as a file plan or business
classification scheme. In its most basic form,
abusiness classification scheme is a list of
activities (for example, finance or HR) arranged
bybusiness functions, however, it is often linked
toan organisation’s hierarchical structure.
Records should be arranged into a classification
scheme, as required by ISO 15489 and Section 46
Code of Practice of the Freedom of Information
Act 2000. At the simplest level, the business
classification scheme can be anything from an
arrangement of files and folders on a network to
an EDRMS. The important element is that there is
an organised naming convention, which is logical,
and can be followed by all sta. The scheme
can be designed in dierent ways. Classification
schemes should try to classify by function first.
Once a recommended functional classification has
been selected, the scheme can be further refined
to produce a classification tree based on function,
activity and transaction, for example:
Function: corporate governance.
Activity: board minutes and associated papers.
Transaction: April 2018 to March 2019.
The transaction can then be assigned a rule
(suchas retention period), a security status or
other action based on the organisational policy.
The scheme will enable appropriate management
controls to be applied and support more accurate
retrieval of information from record systems.
3.6 Using metdt to orgnise
nd find records
Metadata is “data about data” or structured
information about a resource. The Cabinet Oce
e-Government Metadata Standard statesthat:
“metadata makes it easier to manage or find
information, be it in the form of webpages,
electronic documents, paper files or databases
and for metadata to be eective, it needs to be
structured and consistent across organisations”.
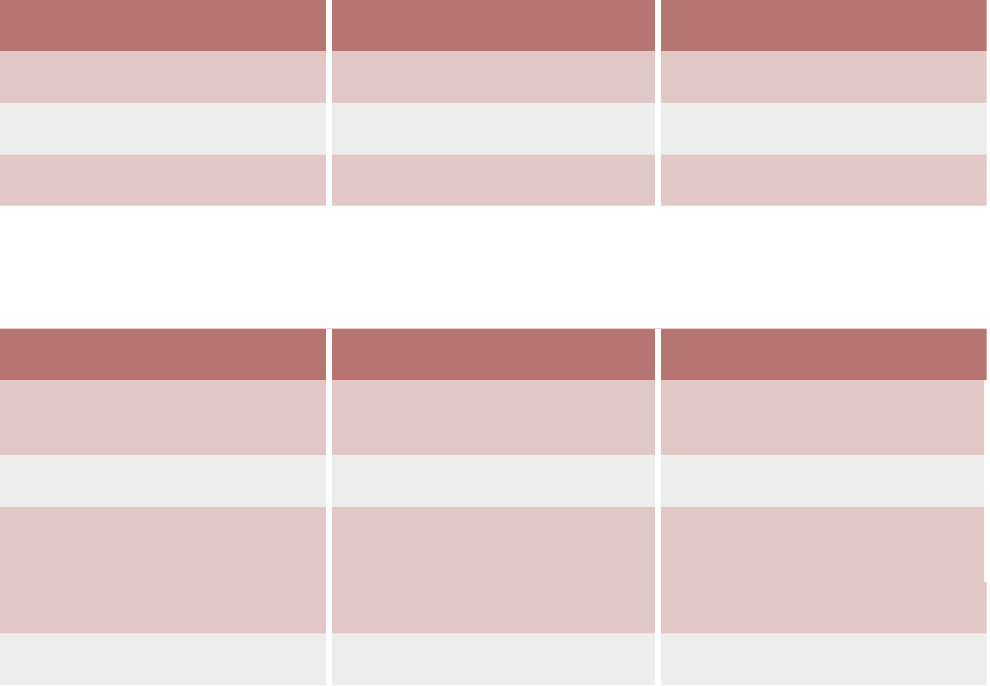
The standard sets out 25 metadata elements,
which are designed to form the basis for the
description of all information. The standard lists
four mandatory elements of metadata that must
be present for any piece of information. A further
three elements are mandatory if applicable and
two more are recommended.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
14
Mandatory elements Mandatory if applicable Recommended
Creator Accessibility Coverage
Date Identifier Language
Subject Publisher
The following provides a practical example of the metadata standard being used to produce a label to be
placed on the side of a box of paper records, which are ready to archive:
Box label Local interpretation Metadata standard
Aneurin Bevan University
HealthBoard
Organisation name Creator
Midwifery Service name Creator
Patient case records surname
A-F
Description of record Subject or title
2000 Date or year of discharge Date
2025 Date or year of destruction Date
Where there is sucient metadata it can be
possible to arrange records by their metadata
alone, however, a business classification scheme
would always be recommended. Records
arranged by their metadata rather than into
a classification scheme often lack context.
Thisreduces the ability to produce an authentic
record. Finding records arranged in this way is
often reliant on a powerful search tool used to
“mine” the data or use a process called “digital
archaeology”. This is not recommended because
it is so time-consuming to determine authenticity,
but it has been included in this Code as legacy
record keeping systems may not have been
organised logically.
3.7 Apping securit
cssifictions
There is no expectation that a security
classification must be applied or used by all
health and care organisations. For example,
itwould be disproportionate for a small care
home or dental practice to apply government
security classifications to a small cohort of records.
Whereas a large NHS Trust may want to use
asecurity classification scheme.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
15
Section 4:
Records storge for
opertion use
4.1 Overview
This section covers how to store records for
operational use. It includes considerations
relating to both paper and digital records
including the challenge of ensuring digital
records remain authentic and usable over
time and the management of o-site storage.
Furtherinformation about the management of
specific formats of records (for example,
cloud-based records and records created on
personally owned computers and equipment)
arein Appendix III.
4.2 Mngement nd storge
ofpper records
Wherever possible, organisations should be
moving to digital records. The original paper
record guarantees the authenticity of the record.
However, it can make it hard to audit access to
the record, depending on where this is stored,
because paper records do not have automatic
audit logs. Storage of paper records also will incur
costs, whether in-house or osite. This cost will
only increase as the size of the holding or length
of time they are stored, increases.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
16
Where possible, paper records management
processes should be as environmentally friendly
as possible. This will help contribute towards
NHS Wales’s target to reduce its carbon footprint
and environmental impact. Examples include the
shredding of paper records and the end product
used for recycling purposes instead of burning
records in industrial furnaces.
4.3 Mngement nd storge
ofdigit records
Digital records oer many advantages over paper
records. They can be accessed simultaneously
by multiple users, take up less physical storage
space and enable activities to be carried out more
eectively, for example, through the use of search
functions and digital tools.
Digital information must be stored in such a way
that, throughout its lifecycle, it can be recovered
in an accessible format in addition to providing
information about those who have accessed
therecord.
The European Commission has produced
an overarching standard in this area.
(Furtherinformation is available on the DLMforum
foundation). The authenticity of a record
isdependent on a number of factors:
• sucient metadata to allow it to remain reliable,
integral and usable (refer to Section 3);
• the structure of the record;
• the business context;
• links between other documents that form part
of the transaction the record relates to.
The management of digital records requires
constant, continual eort, and should not be
underestimated. Failure to properly maintain digital
records can result in doubt being raised over the
authenticity of the digital image. Examples include:
• a record with web links that do not work
once they are converted to another format,
losesintegrity;
• a record with attachments, such as hyperlinks
or embedded documents that do not migrate
to newer media, are not complete or integral;
• an email message that is not stored with the
other records related to the transaction, is not
integral as there are no supporting records to
give it context.
Digital information presents a unique set of issues
which must be considered and overcome to
ensure that records remain:
• authentic;
• reliable;
• retain their integrity;
• retain usability.
Digital continuity refers to the process of
maintaining digital information in such a way that
the information will continue to be available as
needed despite advances in digital technology
and the advent of newer digital platforms.
Digitalpreservation ensures that digital information
of continuing value remains accessible and usable.
The amount of work required to maintain digital
information as an authentic record must not be
underestimated. For example, the information
recorded on an electronic health record
system may need to be accessible for decades
(includingan audit trail to show lawful access and
maintain authenticity) to support continuity of care.
Digitalinformation must not be left unmanaged
in the hope a file can be used in the future.
TheNational Archives has produced a variety of
technical and role-based guidance and useful
checklists to support this management process.
As there are no digital records in existence today
that are of such an age, it is dicult to even plan
continued access in an authentic form over such
atimeframe. For example:
• paper records can deteriorate over time –
socan digital media as the magnetic binary
code can de-magnetise in a process called
“bit rot” leading to unreadable or altered
information, thus reducing its authenticity;

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
17
• software upgrades can leave other applications
unusable as they may no longer run on
updated operating systems;
• media used for storage may become obsolete
or degrade, and the technology required to
read them may not be commercially available;
• file formats become obsolete over time
as more ecient and advanced ones
aredeveloped.
There are several strategies that can be adopted
to ensure that digital information can be kept in
an accessible form over time. Among the most
common strategies adopted are:
• migration to the new systems (retaining existing
formats – this is the preferred method);
• emulation (using software to simulate the
original application);
• preservation of host system;
• conversion to a standard file format
(or a limited number of formats).
The Digital Preservation Coalition has produced
a Digital Preservation Handbook that will help
organisations understand some of the issues
associated with retaining digital records for long
periods of time.
The UK government National Cyber Security
Centre (NCSC) provides good practice guidelines
on forensic readiness and defines it as:
“the achievement of an appropriate level of
capability by an organisation in order for it to be
able to collect, preserve, protect and analyse
digital evidence so that this evidence can be
eectively used in any legal matters, in security
investigations, in disciplinary matters, in an
employment tribunal or in a court of law”.
The NCSC notes that “it is important for each
organisation to develop a forensic readiness of
sucient capability and that it is matched to its
business need”. Forensic readiness involves:
• specification of a policy that lays down a
consistent approach to digital records;
• detailed planning against typical (and actual)
case scenarios;
• identification of (internal or external) resources
that can be deployed as part of those plans;
• identification of where and how the associated
digital evidence can be gathered that will
support case investigation;
• a process of continuous improvement that
learns from experience.
In many organisations, forensic readiness is
managed by information security or informatics
sta, but records managers need to ensure that
they input to policy development and feed in case
scenarios as necessary.
Where possible, electronic records management
processes should be as environmentally friendly
as possible to help contribute towards NHS
Wales’s target to reduce its carbon footprint and
environmental impact. An example would be to
replace outdated IT servers with up to date energy
ecient systems, reducing the amount of energy
required for the solution.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
18
4.4 Mnging osite records
It is vital to highlight the importance of actively
managing records stored osite. This applies
toboth paper records and records stored in
cloud-based solutions (refer to Appendix III for
further information about cloud-based records).
Managing o-site records eectively will
ensurethat:
• there is a full inventory of what is held osite;
• retention periods are applied to each record;
• a disposal log is kept;
• there is evidence of secure disposal of records
and information.
The National Archives has produced guidance
to identify and support the requirements
for ositestorage of physical records and
further guidance on identifying and specifying
requirements for osite storage of physical
records. It is a best practice benchmark for all
organisations creating or holding public records
and provides advice and guidance on the tracking
of records at all stages of the information lifecycle
up to disposal. TheNational Archives does not
provide guidance on onsite storage of operational
and live records. This should be determined by
the local organisation in line with this Code.
When considering using osite storage,
organisations should consider the following:
• Instruction – the controller must provide clear
instructions relating to all processing of osite
records including destruction of the records.
• Access to site – access to the storage site
should be possible to be able to exercise due
diligence, and conduct site visits if necessary.
• Retrieval – organisations will need to agree
how their records will be retrieved and what
timeframe they will be returned. An example
would be to ensure that you can respond to
subject access and FOI requests or retrieve
them to dispose of when the minimum retention
period has been reached.
You must conduct a DPIA if you are looking to
start storing records osite. This is because it will
be a new process for handling potentially high
volumes of personal data with increased risk.
ADPIA must be completed:
• at the outset of entering an osite storage
contract;
• if you have not completed one before on the
service (even if it has been established for
anumber of years);
• if you change service provider;
• if you change how you manage your contract
or elements of it (for example, change from
destruction by pulping to destruction by
shredding);
• if you end the service by bringing it in-house.
If osite storage is currently operated by your
organisation it may be worth conducting a DPIA
to ensure current measures guard against risks to
privacy. A DPIA is also evidence of due diligence,
providing the outcomes are actioned.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
19
Section 5:
Mngement of records
when the minimum
retention period is reched
5.1 Overview
This section covers the management of records
once their business need has ceased and the
minimum retention period has been reached.
Adetailed retention schedule is set out in
Appendix II. This section includes information
on the destruction and deletion of records,
reviewingrecords for continued retention
once their minimum period for retention has
expired, and the selection of records for
permanent preservation. All organisations have
a responsibility to dispose of records at the end
of their lifecycle (usuallythe end of the retention
period).
Welshpublic records bodies as defined GOWA
2006, Section148 have a statutory duty under
PRA 1958 to ensure that records of permanent or
historic value are transferred to a Place of Deposit
(PoD). Information and advice on transfer to a
Place of Deposit is included in thissection.
Appendix I relating to public Inquiries should also
be considered before destroying any records.
5.2 Appris
Appraisal is the process of deciding what to do
with records once their business need has ceased
and the minimum retention period has been
reached.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
20
This can also be known as the disposition of
records. The National Archives has produced
guidance on appraisal.
Appraisal must be defined in a policy and any
decisions must be documented and linked
to a mandate to act (derived from the board).
Anychanges to the status of records must also
be reflected in your organisation’s Record of
Processing Activity. In no circumstances should
a record or series be automatically destroyed
ordeleted.
When appraising records that have come to the
end of their minimum retention period, you should
consider the following:
Ongoing use
You might need to keep the record for longer
than the minimum period for care, legal or audit
reasons. In these cases, you can set an extension
to the minimum period, provided it is justified
andapproved.
Classification of diseases
(based on ICD10 code)
Some health conditions may lend themselves
towards a longer, or extended, retention period.
Operational delivery
The way a service was delivered may have been
pioneering or innovative at the time, which may
justify an extended retention period or long-term
archival preservation.
The way care is delivered
The records may be reflective of health or care
policy at the time.
Series growth
If the records are part of a series that will be
added to (type of record rather than additional
content into existing records), you need to
consider space issues in your local records store
or organisation archive.
For example, continued expansion of a series that
is hardly recalled would not justify an extension to
the retention period.
Recall rates
If a series of records is routinely accessed to
retrieve records, then there may be justification
for extending the retention period due to ongoing
use. Whereas, for a series of records that has a
very low recall rate, continued retention may be
harder to justify.
Historical value
Under the PRA, public bodies are required to
identify records of historical value and transfer
them to a PoD by the time they are 20 years old.
Inmost cases Welsh bodies will transfer their
records to a PoD such as the local archive or
the National Library of Wales. If the record has
potential historical or social value (for example,
innovative new service or treatment or care
delivery method), then consider retaining for
longer than the original retention period. Itwould
also be helpful to have early discussions with
your local PoD about potential accession, even
if the record has ceased to be of operational
value or use. PoDs will not normally accession
records before 20 years retention has passed,
unless there are exceptional circumstances
for early transfer. The PoD must agree to the
transfer PRIOR to it occurring. If early discussion
with the PoD indicates the record (orseries)
will not be accessioned, and you have no
ongoing operational use for the record or series,
then you must securely destroy the record,
andobtain evidence of destruction (for example,
destructioncertificate).
Previous deposits
The records you hold may be a continuation of
a series that has historically been accessioned
by a local PoD. It is important to find out what
has historically been accessioned from your
organisation to the PoD, so that a series of records
remains complete. It is likely that records that add
to an already accessioned series will continue to
be taken by the PoD.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
21
This list is not exhaustive, and organisations may
have bespoke issues to consider as well.
Digital records can be appraised if they are:
• arranged in an organised filing system;
• dierentiated by the year of creation;
• organised by year of closure;
• clear about the subject of the record.
If digital records have been organised in an
eective file plan or an electronic record keeping
system, this process will be made much easier.
Decisions can then be applied to an entire class of
records rather than reviewing each record in turn.
There will be one of three outcomes from
appraisal:
• destroy or delete;
• continued retention – this will require
justification and documented reasons;
• permanent preservation.
All appraisal decisions need to be justified, follow
policy or guidance, and be documented and
approved by the relevant board, committee or
group of the organisation.
5.3 Destroing nd deeting
records
If as a result of appraisal, a decision is made
to destroy or delete a record, there must be
evidence of the decision. It is good practice to get
authorisation for destruction or deletion from an
appointed committee or group with a designated
function to appraise records, working to a policy
or guidelines. Where the destruction or deletion
process is new, or there is a change in the
destruction process (such as a change of provider,
or the method used), a DPIA must be completed
and signed o by the organisation.
Destruction of paper records
Paper records selected for destruction
can be destroyed, subject to following
ISO 15489-1:2016. Destruction can be conducted
in-house or under contract with an approved
osite company. Ifan osite company is used,
the health or care organisation, as the controller,
is responsible for ensuring the provider chosen
to carry out osite destruction meets the
necessary requirements and can evidence this.
This evidence should be checked as part of due
diligence (forexample, ifthe provider says they
have the ISO accreditation, then check with the
ISO). Other diligence activities, such as a site
visit to the contractor, should also be carried out.
Destruction provider companies must provide a
certification of destruction for the bulk destruction
of records. This certification must be linked to a list
of records, so organisations have clear evidence
that particular records have been destroyed.
Records that do not contain personal data or
confidential material can be destroyed in a less
secure manner (such as confidential waste bins
that do not provide certificates of destruction).
Ifindoubt, material should be treated as
confidential and evidentially destroyed. Do not use
the domestic waste or put records on a rubbish
tip to destroy identifiable, confidential material,
because they remain accessible to anyone
who finds them. The British Security Industry
Association (BSIA) has provided a guideon
information destruction.
Destruction of digital records
Destruction implies a permanent action. Fordigital
records “deletion” may not meet the ISO 27001
standard as the information can or may be able
tobe recovered or reversed. Destruction of
digital information is therefore more challenging.
If an osite company is used, the health and
care organisation as the controller should
checkwith the ISO whether the provider meets
the necessary requirements, similar to the process
forthe destruction of paper records.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
22
One element of records management is
accounting for information, so any destruction of
hardware, hard drives or storage media must be
auditable in respect of the information they hold.
An electronic records management system will
retain a metadata stub which will show what has
been destroyed.
The ICO guidance Deleting personal data sets
out that if information is deleted from a live
environment and cannot be readily accessed
then this will suce to remove information for the
purposes of UK GDPR. Their advice is to only
procure systems that will allow permanent deletion
of records to allow compliance with the law.
Electronic systems will vary in their functionality.
They may have the ability to permanently delete
records from the system or not. Where a record
that has reached its retention period and has been
approved for destruction, then the record should
be deleted if the system allows that function.
Aseparate record should be kept of what record
has been deleted.
If a system doesn’t allow permanent deletion,
thenall reasonable eorts must be made to
remove the record from normal daily use. It should
be marked in such a way that anyone accessing
the record can recognise it as a dormant or
archived record. All activity in electronic systems
must be auditable, and (where appropriate) local
policies and procedures should cover archived
digital records.
In relation to FOIA, the ICO guidance ‘Determining
whether information is held’ advises that once the
appropriate limit for costs incurred for that FOI has
been reached, there are no more requirements to
recover information held. The only exemption to
this would be where the organisation is instructed
by a court order.
The following are examples of when information
cannot be destroyed or disposed of:
• If it is subject to a form of access request,
for example, Subject Access Request (SAR),
FOIArequest.
• If it is required for notified legal proceedings,
for example, a court order, or where there is
reasonable prospect of legal proceedings
commencing (an impending court case).
Thisinformation will possibly be required for
the exercising or defending of a legal right
orclaim.
• If it is required for a coroner’s inquest.
• If it is of interest to a public inquiry, for example,
who will issue guidance to organisations on
what kind of records they may require as part
of the inquiry. Once notified, organisations can
re-commence disposal, taking into account
what records are required by the inquiry. If in
doubt, check with the inquiry team.
5.4 Continued retention
The retention periods given in Appendix II are
the minimum periods for which records must be
retained for health and care purposes. In most
cases, it will be appropriate to dispose of records
once this period has expired, unless the records
have been selected for permanent preservation.
Organisations must have procedures and policies
for any instances where it is necessary to maintain
specifically identified individual records, or group
of records (clinical or otherwise) for longer than the
stated minimum, including:
• temporary retention;
• public inquiries;
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
23
• ongoing access request, for example, where
the ongoing processing of an access request
cuts over the minimum retention period
– itwould not be acceptable to dispose
of a record that is part way through being
processed for an access request because the
minimum retention period has been reached;
• where there is a continued business need
beyond the minimum retention period, and this
is documented in local policy.
There will be occasions where care specialties
will create digital records that have dierent
retention periods. For example, a radiology
scan might need to be kept for the minimum of
8 years, and then destroyed as the record is no
longer required. Yet a dierent image for a similar
case may need to be kept for longer due to the
nature of that particular case. In these situations,
organisations can apply dierent retention times
and this should be picked up at the review stage
once the 8 years has expired.
Where records contain personal data, the decision
to retain must comply with UK GDPR. Decisions for
continued retention beyond the periods laid out in
this Code must be recorded, made in accordance
with formal policies and procedures by authorised
sta and set a specific period for further review.
Generally, where there is justification, records may
be retained locally from the minimum period set in
this Code, for up to 20 years from the last date at
which content was added.
NHS Wales’ individual sta and
patientrecords
For NHS Wales’s individual sta and patient
records that have a recommended retention
period beyond 20 years (for example, maternity
records), these can be retained for longer as
specified in Appendix II, in this case for 25 years,
if there is an ongoing operational need to retain.
This may be reflected in an extended retention
period beyond 20 years being mandated by
the Code (such as with the maternity records).
Whereorganisations use this provision locally
toretain records for longer than 20 years,
thismust be documented in published policies.
It must be remembered that in some cases
of health and social care, there may be gaps
between episodes of care. If a patient or service
user begins a new episode of care whilst their
previous record is still within agreed retention
periods, then these episodes of care will link,
andthe retention period will begin again at the
end of the current episode. This may mean that
some or all of the information from the previous
episode will go over a 20-year retention mark,
butthis is acceptable as it links to a more recent
care episode.
Other types of records
For records that are not sta or patient records,
for example, board minutes or records relating
to buildings, a dierent arrangement is in
place. Where a public body needs to keep
any other type of record beyond 20 years,
thenapproval must be sought separately from
theArchivesAdvisory Council.
This is the case even where the recommended
retention period is longer in the Code. The Code
does not recommend a minimum retention period
beyond 20 years for the majority of these types
of records. However asbestos, radiation and
some building records have longer retention
periods due to current legislation at the time of
writing. NHS England are progressing a UK-wide
application to the Advisory Council for these three
types of records. Organisations should retain them
for the retention period set out in the Code at this
time. We will update the Code with the outcome
ofthat application in the next edition of the code.
Organisations should always check current
legislation. Any applications for approval should
be made to The National Archives inthe first
instance by email to asd@nationalarchives.gov.uk.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
24
Information:
Examples of the application of Archives Advisory
Council retention approval
1. A trust wishes to check the retention period
for cancer or oncology records. The Code
states 30years so the records are retained
for 20years without the need to apply the
approval. The last 10 years would be covered
by Archives Advisory Council approval as
they relate to individual patients, providing the
trust has an ongoing need and justification for
continued storage.
2. A trust wishes to retain patient records for
16years due to developments in the treatment
of infectious diseases (where a patient is
cared for in an isolation ward). The Code
recommends eight years before disposal.
Thetrust can make a local decision to retain
the records for 16 years. This does not need
SoS approval because the period is under
20years. The decision is documented in
the trust’s published policy. The trust notes
that retention beyond 20 years for these
records would require Archives Advisory
Council retention approval, subject to ongoing
business need and justification of the proposed
extended retention period.
5.5 Records for permnent
preservtion
The Public Records Act 1958 requires
organisations to select records for permanent
preservation. Selection for transfer under this
Actis separate to the operational review of
records to support current service provision.
It is designed to ensure the permanent
preservation ofa small core (typically 2-5%)
of key records, which will:
• enable the public to understand the working
of the organisation and its impact on the
population it serves;
• preserve information and evidence likely to
have long-term research or archival value.
Records for preservation must be selected in
accordance with the guidance contained in this
Code. Any supplementary guidance issued by
The National Archives and local guidance from
the relevant PoD should always be consulted
in advance of any possible accession. This is to
ensure it is appropriate to transfer the records
selected. Further guidance on selecting relevant
records for permanent preservation can be found
in Welsh Health Circular WHC (2000) 71 and in
the Brief Guide to Transferring Records of Local
Interest to a Place of Deposit.
As a rule, national organisations, will accession
their records to The National Archives, and local
Health boards, trusts and social care organisations
will accession their records to the local PoD within
Wales, as appointed by the Secretary of State
for Culture, Media and Sport. If you are unsure
where you should accession records, contact
the Archives Sector Development Team at TNA.
There is also an app to help bodies identify their
PoD: Where do I deposit my records?
Selection may take place at any time in advance
oftransfer. However, the selection and transfer
must take place at or before records are
20years old. Records may be selected as a class
(forexample, all board minutes) or at lower levels
down to individual files or items.
Records can be categorised as follows:
• transfer to PoD: this class of records should
normally transfer in its entirety to the PoD –
trivial or duplicate items can be removed prior
to transfer;
• consider transfer to PoD: all, some or none
ofthis class may be selected (as agreed with
the PoD);
• no PoD interest.
Other records should not normally be selected
for transfer. Whilst there may be occasions where
records to support research are transferred
(forexample, to support research into rare
conditions), records should not be transferred
just because they relate to research or with the
sole purpose of preservation in case they could
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
25
be used for future research. The Public Records
Act 1958 is not designed to support the routine
archival of research records. Records should not
be transferred unless they specifically meet the
criteria below. If in doubt, it is recommended to
check with the local PoD.
Where it is known that particular records will
be transferred to PoDs routinely, this should
be noted in the records management policy
(orequivalent) alongside the reason for the
routine transfer. Likewise, one-o transfers should
also be noted for reference. It is not practical to
update local policies each time a transfer is made.
Ifa particular type becomes a regular transfer,
this could be added to the next update of the
records management policy. It may be sucient
to publish a link to the PoD’s public catalogue or
The National Archives Catalogue to which data for
transferred records is added annually. Where it is
known a record will form part of the public record
at creation, it must be preserved locally until such
time it can be transferred. PoDs will know which
types of records they will always take (such as
board minutes). The National Archives is working
on providing guidance on which record will always
be transferred and those that might be of local
interest.
Where a clinician has amassed a lifetime of
research or important cases these may be
identified and retained.
Patient or service user records for
permanent preservation
Records of individual persons may also be
selected and transferred to the PoD provided this
is necessary and proportionate in relation to the
broadly historical purposes of the Public Records
Act 1958 and PoD agreement. For example,
individual patient files relating to a hospital that is
now closed and the files are coming to the end
oftheir retention can be oered.
Patient or service user confidentiality will normally
prevent use for many decades after transfer
and the physical resource will be substantial
(forexample, x number of archive boxes) therefore
the transfer of patient or service users records
should only be considered where one or more
ofthe factors listed below apply:
• the organisation has an unusually long or
complete run of records of a given type;
• the records relate to population or
environmental factors peculiar to the locality;
• the records are likely to support research into
rare or long-term conditions;
• the records relate to an event or issue of
significant local or national importance;
• the records relate to the development of
new or unusual treatments or approaches to
care, orthe organisation is recognised as a
national or international leader in the field of
medicine or care concerned;
• the records throw particular light on the
functioning, or failure, of the organisation,
orNHS Wales or social care in general;
• the records relate to a significant piece
ofpublished research.
Any policy to select patient or service user
records should only be agreed after consultation
with appropriate clinicians, the group or
committee responsible for records management
and (ifnecessary), the Caldicott Guardian.
Thisdecision, and the reasoning behind the
decision, should be published in the minutes
of the meeting at which this decision is taken.
Routine transfers of patient or service user
records to a PoD can be included in the records
management policy of the organisation or its
equivalent.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
26
Any records selected should normally be retained
within NHS Wales or social care (under the terms
of Retention Instrument 122) until the patient
or service user is deceased, or reasonably
assumed to be so and then can subsequently be
transferred. Records no longer required for current
service provision may be temporarily retained
pending transfer to a PoD. Records containing
sensitive or confidential information should not
normally be transferred early, unless in agreement
with the PoD. If a patient or service user expresses
a wish that they do not want their health or
care record transferred to a PoD, this must be
respected unless the transfer is required by law.
Transfers of records to the Place of Deposit
Records selected for permanent preservation
should be transferred to the relevant PoD
appointed by the Secretary of State for Digital,
Culture, Media and Sport. PoDs are usually public
archive services provided by the relevant local
authority. Current contact details of PoDs and
the organisations which should transfer to them
can be found on The National Archives website.
Further guidance for transferring records to a
PoD can also be found on The National Archives
website.
As a general rule, national public sector
organisations will deposit with The National
Archives, while local organisations will deposit
with a local PoD. This could be the county
record oce, or a specialised facility run by
local authorities for the county. For example,
SwanseaBay University Health Board deposits its
records to the West Glamorgan Archive Service.
There will be a mandatory requirement to
transfer some types of records whereas others
will be subject to local agreement. The retention
schedule included with this Code identifies
records which should be transferred to the locally
approved PoD when business use has ceased.
There may also be records of local interest which
need to be accessioned to the PoD (such as a
continuation of a series already accessioned).
Priorto any transfer being made, a discussion
must be had with the local PoD to enable
agreement on which records will be transferred
and the process for doing so. (Alsorefer to
Appendix I, which provides information about
public inquiries that may impact upon the
selection of records for transfer).
Transferred records should be in good condition
and appropriately packed, listed and reviewed
for any FOIA exemptions. Records selected
for transfer to a PoD (after appraisal) may
continue to be exempt from public access for
a specified period after transfer in accordance
with Section 66 of FOIA. For more detail on the
transfer process and sensitivity review refer to
TheNational Archives guidance.
Requests to access records held in the
Place of Deposit (PoD)
Once transferred to the PoD, records will still
be owned by the organisation transferring them
and all relevant laws will apply. Individual records
deposited with PoDs are still protected by the
UK GDPR, FOIA and duty of confidentiality.
Whererecords are kept for permanent
preservation for reasons other than care,
consideration should be given to preserving
the records in an anonymised way to protect
confidentiality. Where this is not possible,
thenconsider removing as many identifiers as
possible. If you are looking to preserve a record
because the treatment provided was innovative
orhighlights new ways of working, then the
identity of the patient is not required. For individual
care, itwould be required, as the record may need
to be retrieved.
Where a local PoD holds records and access is
requested, the PoD will liaise with the depositing
organisation before releasing any information
(including any checks for SARs required by
UK GDPR and any exemptions under FOIA).
Thisallows for a check for any harmful information
that may be in the record or if there are other
grounds on which to withhold the record. Where
a public interest test is required, thetransferring
organisation must carry this outand inform the
PoD of the result.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
27
The depositing organisation must make a decision
on what information to release and where
information is withheld, explain the reason why
(except in exceptional circumstances, for example,
a court order to the PoD).
Unless there are exceptional circumstances,
PoDswill not normally continue to apply FOI
exemptions to records more than 100 years old.
Where a patient or service user has died the
UK GDPR no longer applies but FOIA applies
regardless as to whether the individual is alive
or not. The Section 41 (confidence) exemption of
FOIA and the duty of confidence remain relevant
so records cannot be accessed byanyone
who does not have a lawful basis to view a
record. FOIA decisions indicate that, ingeneral,
healthand social care information will remain
confidential after death.
The duty of confidence does diminish over time,
but it is recommended that at least 10 years
should have passed after a person’s death
before reviewing the consequences of relaxing
disclosure controls on information about a person
previously regarded as confidential. This review
should consider the potential harm or distress to
surviving family members of disclosing information
that might be regarded as particularly sensitive
or likely to attract publicity, and the risks that
the disclosure might undermine public trust in
the health and care system. When a person
is deceased, theAccess to Health Records
Act1990 may enable access to the health record
for a limited purpose by specified individuals
(suchasthose with a claim arising out of the death
of the person).

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
28
Appendix I:
Pubic nd sttutor
inquiries
Records form an important part of the evidence
in inquiries. Inquiries take into account a huge
range of records and what is required can
vary byinquiry. When an inquiry is conducted,
theinquiry team will issue detailed guidance
setting out what types of records they are
interested in. If you have any records that an
inquiry requests, you must produce them or
explain why you cannot produce them.
Before any records relating to inquiries are
destroyed, you must check with the inquiries
team that they are no longer required. If you are
indoubt regarding records that may or may not
be of use for an inquiry, you must retain them until
there is clear instruction from the inquiry.
Before considering the selection of records for
permanent preservation under the Public Records
Act 1958 (refer to Section 5), you should discuss
any inquiries with the relevant PoD to take account
of exceptional local circumstances and defunct
record types not listed here.
At the time of writing there are two independent
inquiries which have requested that large parts
ofthe health and social care sector do not destroy
any records that are, or may fall into the remit of
the inquiry:
• The Independent Inquiry into Child Sexual
Abuse (IICSA) – this is due to finish in 2022.
Records that should not be destroyed include
children’s records and any instances of
allegations or investigations or any records
ofan institution where abuse has or may
haveoccurred.
• The Infected Blood Inquiry – further
information about the records required can be
found on their website.
The UK Government has also committed to
holding a public inquiry into its response to the
coronavirus pandemic that began in March 2020.
No details of what records will be required are
known at this stage, but it is likely to require
records relating to policy and decision making
asaminimum.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
29
Appendix II:
Retention schedue
This appendix sets out the retention period for
dierent types of records relating to health and
care. Where indicated, Appendix III should also be
referred to. This sets out further detail relating to
the management of specific types and formats of
records. An easily searchable version of this table
can also be found online here.
The following information is important
to ensure the retention schedule is
usedcorrectly
The retention periods listed in this retention
schedule must always be considered the minimum
period. With justification, a retention period can
be extended for the majority of cases, upto
20years (refer to Section five of the Code).
Formore information, refer to R v Northumberland
County Council and the Information Commissioner
(23July 2015). It is legitimate to vary common
practice or guidance where a well-reasoned
casefor doing so is made.
Retention periods begin when the record ceases
to be operational. This is usually at the point of
discharge from care when the record is no longer
required for current on-going business, or the
patient or service user has died. There are some
exceptions to this rule, whereby the retention
begins from the date the record is created
(forcorporate records, such as policies, the
retention may start from the date of publication).
These are marked with an asterisk (*) in the
schedule and may also contain further information
in the notes for that entry.
If a record comes back into use during its retention
period, then the retention period will reset and
begin again from the end of the second period
of use.
This may mean that records will look as if they
are being kept for longer than the retention
times stated here, or even maximum periods as
suggested by law, but this is acceptable where
retention periods reset due to use (refer to
sectionfive of the Code).
The actions following review as set out in the
schedule are as follows:
Review and destroy if no longer required
Destroy refers to the confidential and secure
destruction of the record with proof of destruction.
These will be records with no archival value and
there is no longer an ongoing business need to
retain them for longer.
Review and dispose of if no longer required
“Dispose of” refers to the secure destruction
of arecord OR the transferral to the appointed
PoD for permanent preservation. A certificate
of transfer will be provided as proof of transfer
(andcan act as evidence of disposal). Refer to
Section five of the Code for further information
about permanent preservation.
Review and consider transfer to PoD
This refers to records that are more likely to be
transferred to the PoD, subject to their discussion
and agreement about potential accession.
Not all records considered for accession will
be taken by the PoD. If the record has been
oered and declined to be taken, and it has no
further retention value, then it must be securely
destroyed. Where you have potentially a new
series of records for the PoD, you must discuss
accessioning them before any action is taken.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
30
Review and transfer to PoD
This refers to records that should be transferred
to the PoD such as trust board minutes and final
annual financial report – local agreement will
already be in place to accession these.
It is very important that any health and care
records are reviewed before they are destroyed.
This review should take into account:
• serious incidents which will require records
to be retained for up to 20 years as set out
intheschedule;
• use of the record during the retention period
which could extend its retention;
• potential for long-term archival preservation
– this may particularly be the case where
the records relate to rare conditions such
as Creutzfeldt-Jakob Disease records or
innovative treatments, for example,
new cancer treatments.
If setting a retention period not covered by
this Code, there are a number of factors to
considerincluding:
Legal or regulatory obligations
There may be a specific legal or regulatory
reason to keep a record, which may also provide
guidance on how long that record needs to be
kept to meet that obligation.
Purpose of the record
The reasons you have created the record may
also help define how long you need to keep them
for. A record created for medico-legal reasons may
need to be for a long period of time, whereasa
record created for a specific event that has no
post-event actions will attract a short retention
period.
Number of records
The number of records in a series can help you
set a retention period. It is worth noting that the
number of records is not directly proportionate to
a longer retention period (for example, the more
records created, then the longer they must be
kept). It should also be noted that the number of
records is also not indicative of historical value.
Due to its type, one record may have historical
value, where a series of 200+ records might not.
Service delivery
The uniqueness or niche way a service is
delivered may lend itself to a longer retention
period. PoDs can be interested in taking records
relating to services that were delivered in a
uniqueway.
Call or recall of records
If a record or series has a low recall rate, it could
be indicative of a shorter retention period.
Likewise records that are continually in use may
require a longer retention period.
The above list is not exhaustive.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202231
Care records
Record type Retention
period
Disposal action Notes
Adult health records not
covered by any other section
in this schedule (includes
medical illustration records
such as x-rays and scans
as well as video and other
formats. Also includes care
plans).
8 years. Review and consider transfer
to PoD.
Records involving pioneering or innovative treatment
may have archival value, and their long term preservation
should be discussed with the local PoD or The National
Archives.
Also refer to Appendix III: ambulance service records.
Adult social care records
(including care plans).
8 years. Review and destroy if no
longer required.
Children’s records (including
midwifery, health visiting and
school nursing): can include
medical illustrations, as well
as video and audio formats.
Up to 25th or
26th birthday.
Review and destroy if no
longer required.
Retain until 25th birthday, or 26th if the patient was 17
when treatment ended.
Clinical records that pre-date
the NHS (July1948).
Review and transfer to PoD. Contact your local PoD to arrange review and transfer.
Records not selected by the PoD must be securely
destroyed.
Dental records:
clinical care records.
15 years. Review, and destroy if no
longer required.
Based on Limitations Act 1980. This applies to all dental
care settings and the NHS BSA. This also includes FP17
orFP17O forms.
Dental records:
finance related.
2 years. Review, and destroy if no
longer required.
These include PR forms. NHS BSA may retain financial
records for a minimum 6 years.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202232
Record type Retention
period
Disposal action Notes
Electronic Patient Record
Systems (EPR).
Refer to notes. Review and destroy if no
longer required.
Where the system has the capacity to destroy records in
line with the retention schedule, and where a metadata
stub can remain, demonstrating the destruction, then the
Code should be followed in the same way for digital as
well as paper records with a log kept of destruction.
If the EPR does not have this capacity, then once
records reach the end of their retention period,
theyshould be made inaccessible to system users upon
decommissioning. The system, along with the audit trails,
should be retained for the retention period of the last
entry related to the schedule.
When considering new systems, data controllers should
consider that commissioning systems with limited storage
breaches UK GDPR, and new systems should have
capacity to comply with UK GDPR.
GP patient records:
deceased patients.
10 years. Review and destroy if no
longer required.
Confidentiality generally continues after death and
records should be retained for medico-legal and
possible public interest, for example, research reasons.
Reviewretention after 10 years when possible
medico-legal reasons will lapse under requirements
of the Limitation Act 1980. Destroy if the record holds
no value for researchers. Also refer to Appendix III:
GPrecords.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202233
Record type Retention
period
Disposal action Notes
GP patient records:
livingpatients.
Continual
retention.
If the patient has not been seen for 10 years, or a request
for transfer to a new GP has not been received, theGP
practice should check the Wales Demographics Service
(WDS) for indication of death or other reason for no
contact. If there is no reason to suggest no contact,
then the record must be kept by the GP practice.
Theserecords cannot be disposed of as they may require
further services as they get older.
If they have died, or transferred to a new practice,
transferthe record to Primary Care Services in NHS
Wales Shared Services Partnership (NWSSP) or the
new provider respectively. Also refer to Appendix III:
GPrecords.
GP patient records:
de-registered cases where
the reason is unknown.
100 years. Review and dispose of if no
longer required.
These are cases where the patient has de-registered
from the practice, but the reason is unknown. It would
be good practice for GPs to check if there is a reason
for de-registration (death, missed registration at another
practice, emigration etc.). It is not suggested that a
retrospective check be carried out, but it would be
goodpractice going forward to conduct a check for
thesecases.
Once checked under General Medical Services
(GMS) regulations, records should be sent to NHS
Wales’ Primary Care Services in NWSSP. (Also refer to
AppendixIII: GP records.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202234
Record type Retention
period
Disposal action Notes
GP patient registrations form. 6 years after
the year of
registration.
Review and dispose of if no
longer required.
These need to be kept for 6 years as GP per capita
payments are made based on registered patient
numbers. Most GP practices scan the form into the
patient’s electronic record once it is created. The paper
form can be destroyed securely once the minimum
retention period has been reached, unless there is
another reason to keep the form longer, this would be
identified at the review stage.
Integrated records:
allorganisations contribute
to the same single instance
of the record.
Retain for
period of
longest
specialty.
Review and consider transfer
to PoD.
The retention time will vary depending upon which type
of health and care settings have contributed to the record.
Areas that use this model must have a way of identifying
the longest retention period applicable to the record.
Integrated records:
allorganisations contribute
to the same record, but keep
alevel of separation
(refer to notes).
Retain for
relevant
specialty
period.
Review and consider transfer
to PoD.
This is where all organisations contribute into the same
record system but have their own area to contribute to
and the system still shows a contemporaneous view of
the patient record.
Integrated records:
allorganisations keep their
own records, but enable
them to be viewed by other
organisations.
Retain for
relevant
specialty
period.
Review and consider transfer
to PoD.
This is the most likely model currently in use.
Organisations keep their own records on their patients
or service users but can grant ‘view only’ access to other
organisations, to help them provide health and care to
patients or service users.
Mental health records
including psychology
records.
20 years,
or10years after
death.
Review and consider transfer
to PoD.
Covers records made under the Mental Health Act (MHA)
1983 and 2007 amendments.
Records retained solely for any person who has been
sectioned under MHA1983 must be considered for longer
than 20 years where the case is ongoing, or the potential
for recurrence is high, based on local clinical judgment.
This applies to records of patients or service users,
regardless of whether they have capacity or not.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202235
Record type Retention
period
Disposal action Notes
Obstetrics, maternity,
antenatal and postnatal
records.
25 years. Review and destroy if no
longer required.
For record keeping purposes, these are considered to be
as much the child’s record as the parent, so the longer
retention period should be considered.
Prison health records. 10 years. Review and destroy if no
longer required.
A summary of their prison healthcare is sent to the
person’s new GP upon release and the record should
beconsidered closed at the point of release.
These records are unlikely to have long term archival
value and should be retained by the organisations
providing care in the prison, or successor organisations
ifthe running of the service changes hands.
Cancer/oncology records:
any patient*.
30 years, or
8 years after
death.
Review and consider transfer
to PoD.
Retention for these records begins at diagnosis rather
than the end of operational use. For clinical care reasons,
these records must be retained longer in case of
re-occurrence. Where the oncology record is part of the
main records, then the entire record must be retained.
Contraception,
sexual health,
familyplanning,
Genito-Urinary Medicine
(GUM).
8 or 10 years. Review and destroy if no
longer required.
8 years for the basic retention requirement but this is
increased to 10 in cases of implants or medical devices.
If the record relates to a child, then retain in line with
children’s records.
(Also refer to Appendix III: records dealt with under the
NHS Trusts and Primary Care Trusts (Sexually transmitted
disease) directions 2000.
Creutzfeldt-Jakob Disease:
patient records.
30 years or
10 years after
death.
Review and consider transfer
to PoD.
Diagnosis records must be retained for clinical care
purposes.
Human Fertility and
Embryology Authority (HFEA)
records: treatment provided
in licenced centres.
3, 10,
30 or 50years.
Review and destroy if no
longer required.
These retention periods are set out in HFEA guidance.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202236
Record type Retention
period
Disposal action Notes
Long-term illness,
orillness that may reoccur:
patientrecords.
20 years,
or10years
afterdeath.
Review and destroy if no
longer required.
Necessary for continuation of clinical care. The primary
record of the illness and course of treatment must be kept
where the illness may reoccur or it is a life-long condition
such as diabetes, arthritis or Chronic Obstructive
Pulmonary Disease.
Sexual Assault Referral
Centres (SARC).
30 years,
or 10 years
after death
(ifknown).
Review, and destroy if no
longer required.
These records need to be kept for medico-legal reasons
because an individual may not be in a position to bring
a case against the alleged perpetrator for a long time
after the event. Once the retention period is reached,
adecision needs to be made about continued retention.
Records cannot be kept indefinitely just in case an
individual might bring a case. Some individuals may never
bring a case and indefinite retention may be seen as a
breach of UK GDPR, keeping information longer than
necessary. Consideration also needs to be given to the
Police and Criminal Evidence Act 1984, Human Tissue
Act 2004, and Criminal Procedure and Investigations
Act1996 legal requirements; other laws and regulations
may also need to be taken into account.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202237
Pharmacy
Record type Retention
period
Disposal action Notes
Controlled drugs: registers. 2 years,
refer to notes.
Review and destroy if no
longer required.
Misuse of Drugs Act 2001.
The Controlled Drugs (Supervision of Management and
Use) (Wales) Regulations 2008.
Also refer to Appendix III: controlled drugs.
Controlled drugs: order
books, requisitions etc.
2 years. Review, and destroy if no
longer required.
Misuse of Drugs Act 2001.
The Controlled Drugs (Supervision of Management and
Use) (Wales) Regulations 2008.
Pharmacy prescription
records.
2 years. Review and destroy if no
longer required.
A record of the prescription will also be held by NWSSP
and their Primary Care Services and there will be an
entry on the patient record. Further advice and guidance
on pharmacy records can be found on the Specialist
Pharmacy Service website.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202238
Pathology
Record type Retention
period
Disposal action Notes
Pathology reports,
information about samples.
Refer to notes. Review and consider transfer
to PoD.
This Code is concerned with the information about a
specimen or sample. The length of time clinical material
(for example, a specimen) is stored will drive how long
the information relating to it is retained. Sample retention
can be for as long as there is a clinical need to hold it.
Reportsshould be stored on the patient file.
It is common for pathologists to hold duplicate records.
For clinical purposes, these should be retained for
8years after discharge or until a child’s 25thbirthday.
Ifinformation is retained for 20 years, it must be
appraised for historical value, and a decision made about
its disposal. (Also refer to Appendix III – specimens
andsamples).
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202239
Event and transaction records
Record type Retention
period
Disposal action Notes
Blood bank register*. 30 years
minimum.
Review and consider transfer
to PoD.
Need to be disposed of if there is no on-going need to
retain them, such as the currently ongoing Infected Blood
Inquiry, subject to any transfer to the PoD.
Clinical audit*. 5 years. Review and destroy if no
longer required.
Five years from the year in which the audit was
conducted.
Chaplaincy records*. 2 years. Review and consider transfer
to PoD.
Also refer to corporate governance records.
Clinical diaries. 2 years. Review and destroy if no
longer required.
Two years after the year to which they relate. Diariesof
clinical activity and visits must be written up and
transferred to the main patient record. If the information
is not transferred from the diary, so the only record of the
event is in the diary, then this must be retained for eight
years and reviewed. Some sta keep hardback diaries
of their appointments or business meetings. If these
contain no personal data, they can be disposed of after
twoyears.
Clinical protocols*. 20 years. Review and consider transfer
to PoD.
Clinical protocols may have preservational value.
Theymay also be routinely captured in clinical
governance meetings which may form part of the
permanent record, refer to corporate governance records.
Datasets released by DHCW
and its predecessors.
Delete with
immediate
eect.
Delete in line with DHCW
instructions.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202240
Record type Retention
period
Disposal action Notes
Destruction certificates,
or electronic metadata
destruction stub, or record of
clinical information held on
physical media.
20 years. Review and consider transfer
to PoD.
Destruction certificates created by public bodies are not
covered by a retention instrument; if they do not relate
to patient care and if a PoD or The National Archives do
not accession them. They need to be destroyed after
20years.
Equipment maintenance
logs.
11 years. Review and destroy and no
longer required.
General ophthalmic services:
patient records related to
NHS financial transactions.
6 years. Review and destroy if no
longer required.
GP temporary resident forms. 2 years. Review and destroy if no
longer required.
This assumes acopy has been sent to the responsible
GPfor inclusion in the GP patient record.
Inspection of equipment
records.
11 years. Review and destroy if no
longer required.
Notifiable diseases book*. 6 years. Review and destroy if no
longer required.
Operating theatre records. 10 years. Review and consider transfer
to PoD.
10 years from the end of the year to which they relate.
Patient property books. 2 years. Review and destroy if no
longer required.
Two years from the end of the year to which they relate.
Referrals: NOT ACCEPTED. 2 years. Review and destroy if no
longer required.
Retention period begins from the DATE OF REJECTION.
These are seen as an ephemeral record.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202241
Record type Retention
period
Disposal action Notes
Requests for care funding:
NOT ACCEPTED.
2 years. Review and destroy if no
longer required.
Retention period begins from the DATE OF REJECTION.
These are seen as an ephemeral record.
Please note: These may have potential PoD interest as
what NHS Wales or social care can or cannot fund can
sometimes be an issue of local or national significance
and public debate. Refer to Appendix III: individual
funding requests.
Screening*: including
cervical screening; where no
cancer or illness detected is
returned.
10 years. Review and destroy if no
longer required.
Where cancer is detected, refer to the cancer or oncology
schedule.
Screening: children. 10 years or
25thbirthday.
Review and destroy if no
longer required.
Treat as a child health record and retain for either 10 years
or up to 25th birthday, whichever is the LONGER.
Smoking cessation. 2 years. Review and destroy if no
longer required.
Retention begins at the end of the 12-week quit period.
Transplantation records*. 30 years. Review and consider transfer
to PoD.
Refer to guidance issued by the Human Tissue Authority.
Ward handover sheets*. 2 years. Review and destroy if no
longer required.
This information relates to the ward. Any individual sheets
held by sta may be destroyed confidentially at the end
of the shift.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202242
Telephony systems and services
This is related to 111 or 999 phone calls or services, Ambulance, out of hours, and single point of contact call centres.
Record type Retention
period
Disposal action Notes
Recorded conversations:
which may be needed later
for clinical negligence or
other legal purposes*.
6 years. Review and destroy if no
longer required.
Retention period runs from the date of the call and is
intended to cover the Limitation Act 1980.
Recorded conversations:
which form part of the
healthrecord*.
Treat as a
health record.
Review and destroy if no
longer required.
It is advisable to transfer any relevant information into
the main record, through transcription or summarisation.
Call handlers may perform this task as part of the call.
Where it is not possible to transfer clinical information
from the recording to the record, the recording must
be considered as part of the record and be retained
accordingly.
Telephony systems record*. 1 year. Review and destroy if no
longer required.
This is the minimum specified to meet NHS contractual
requirements.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202243
Births, deaths and adoption records
Record type Retention
period
Disposal action Notes
Birth notification to child
health.
25 years. Review and destroy if no
longer required.
Retention begins when the notification is received by the
child health department. Treat as part of the child’s health
record if not already stored within the health record.
Birth registers*. 2 years. Review and consider transfer
to PoD.
Where registers of all births that have taken place in a
particular hospital or birth centre exist, these will have
archival value and should be retained for 25 years and
oered to the local PoD at the end of the retention period.
Information is also held by the Welsh Birth Notification
Service electronic system, and by ONS. Other information
about a birth must be recorded in the care record.
Body release forms*. 2 years. Review and destroy if no
longer required.
Death – cause of death
certificate counterfoil*.
2 years. Review and destroy if no
longer required.
These detail the name of the deceased and suspected
cause of death (which initially may be dierent to the
final cause of death as stated on the ocial death
certificate). A death notification certificate is issued if a
doctor is satisfied there is no suspicious or unexpected
circumstances surrounding the death, and the counterfoil
retained by the setting that issued the initial cause of
death certificate (which is used to obtain the full death
certificate from a registrar of births, death and marriages).
Cases referred to the coroner would not be able to issue
a certificate as the cause would be unknown. These are
unlikely to have archival value.
Death – register information
sent to the general registry
oce on a monthly basis*.
2 years. Review and consider transfer
to PoD.
A full dataset is available from ONS.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202244
Record type Retention
period
Disposal action Notes
Local authority adoption
record (usually held by
theLA)*.
100 years. Review and consider transfer
to PoD.
The local authority Children’s Social Care Team
hold the primary record of the adoption process.
Considertransferring to PoD only if there are known
gapsin the primary local authority record, or the records
pre-date 1976.
Also refer to Appendix III: adoption records.
Mortuary records of
deceased persons.
10 years. Review and consider transfer
to PoD.
Retention begins at the end of the year to which
theyrelate.
Mortuary register*. 10 years. Review and consider transfer
to PoD.
NHS medicals for adoption
records*.
8 years or
25thbirthday.
Review and consider transfer
to PoD.
The health reports will feed into the primary record held
by the local authority. This means that adoption records
held in NHS Wales relate to reports that are already kept
in another file, which is kept for 100 years by the relevant
agency or local authority. Consider transferring to PoD
only if there are known gaps in the primary local authority
record or the records pre-date 1976.
Also refer to Appendix III: adopted persons health
records.
Post-mortem records*. 10 years. Review and destroy if no
longer required.
The coroner will maintain and retain the primary
post-mortem file including the report.
Hospital post-mortem records will not need to be kept
forthe same extended time period as subject to local
policy these reports may also be kept in the medical file.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202245
Clinical trials and research
Record type Retention
period
Disposal action Notes
Advanced medical therapy
research: master file.
20 years. Review and consider transfer
to PoD.
Clinical trials: applications
forethical approval.
5 years. Review and consider transfer
to PoD.
Master file of a trial authorised under the European portal,
under Regulation 536/2014.
For clinical trials records retention refer to the
MHRAguidance. The sponsor of the study will be
the primary holder of the study file and associated
data. Thisis based on the Medicines for Human
Use (ClinicalTrials) Amendment Regulations 2006,
specificallyRegulations 18 and 28).
European Commission
Authorisation (certificate or
letter) to enable marketing
and sale within EU member
state’s area.
15 years. Review and consider transfer
to PoD.
Research: datasets. No longer than
20 years.
Review and consider transfer
to PoD.
Research: ethics committee’s
and HRA approval
documentation for research
proposal and records to
process patient information
without consent.
5 years. Review and consider transfer
to PoD.
This applies to trials where opinions are given to proceed
with the trial, or not to proceed. These may also have
archival value.
Research: ethics committee’s
minutes (including records to
process patient information
without consent).
20 years. Review and consider transfer
to PoD.
Retention period begins from the year to which they relate
and can be as long as 20 years. Committee minutes must
be transferred to PoD.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202246
Corporate governance
Record type Retention
period
Disposal action Notes
Board meetings*. Up to 20 years. Review and transfer to PoD. A local decision can be made on how long to retain the
minutes of board meetings, and associated papers linked
to the board meeting, but this must not exceed 20 years,
and will be required to be transferred to the local PoD or
The National Archives for National Bodies.
Board meetings: closed
boards*.
Up to 20 years. Review and transfer to PoD. Although these may still contain confidential or sensitive
material, they are still a public record and must be
transferred at 20 years, and any FOI exemptions noted,
orindications that the duty of confidentiality applies.
Chief Executive records*. Up to 20 years. Review and transfer to PoD. This may include emails and correspondence where they
are not already included in board papers.
Committees: major, listed
in Scheme of delegation or
report direct into the board,
including major projects*.
Up to 20 years. Review and transfer to PoD.
Committees: minor, not listed
in scheme of delegation*.
6 years. Review and consider transfer
to PoD.
Includes minor meetings, projects, and departmental
business meetings. These may have local historical value
required transfer consideration.
Corporate records of health
and care organisations and
providers that pre-date the
NHS, July 1948.
Review, and transfer to PoD. Contact your local PoD to arrange review and transfer.
Records not selected by the PoD must be securely
destroyed. An example might be the minutes of the
hospital board from 1932, or midwifery diaries dated
December1922.
Data Protection Impact
Assessments (DPIAs).
6 years. Review and destroy if no
longer required.
Should be kept for the life of the activity to which it
relates, plus six years after that activity ends. If the DPIA
was one-o, then 6 years from completion.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202247
Record type Retention
period
Disposal action Notes
Destruction certificates or
record of information held on
destroyed physical media.
20 years. Review and dispose of if no
longer required.
Where a record is listed for potential transfer to PoD
have been destroyed without adequate appraisal,
consideration should be given to a selection of these
asan indicator of what has not been preserved.
Electronic metadata
destruction stubs.
Refer to destruction certificates.
Incidents: serious. 20 years. Review and consider transfer
to PoD.
Retention begins from the date of the Incident; not when
the incident was reported.
Incidents: not serious. 10 years. Review and destroy if no
longer required.
Retention begins from the date of the incident; not when
the incident was reported.
Incidents: serious incidents
requiring investigation.
20 years. Review and consider transfer
to PoD.
These include independent investigations into incidents.
These may have permanent retention value so consult
with the local PoD. If they are not required, then destroy.
Non-clinical QA records. 12 years. Review and destroy if no
longer required.
Retention begins from the end of the year to which the
assurance relates.
Patient advice and liaison
service (PALS) records.
10 years. Review and destroy if no
longer required.
Retention begins from the close of the financial year to
which the record relates.
Patient surveys: individual
returns and analysis.
1 year after
return.
Review and destroy if no
longer required.
May be required again if analysis is reviewed.
Patient surveys: final report. 10 years. Review and consider transfer
to PoD.
Organisations may want to keep final reports for longer
than the raw data and analysis, for trend analysis over
time. This period can be extended, provided there is
justification and organisational approval.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202248
Record type Retention
period
Disposal action Notes
Policies, strategies and
operating procedures,
including business plans*.
Life of
organisation
plus 6 years.
Review and consider transfer
to PoD.
Retention begins from when the document is approved,
until superseded. If the retention period reaches 20 years
from the date of approval, then consider transfer to PoD.
Quarterly reviews from NHS
health boards and trusts.
6 years. Review and destroy if no
longer required.
Retention period in accordance with the Limitation
Act1980.
Risk registers. 6 years. Review and destroy if no
longer required.
Retention period in accordance with the Limitation Act
and corporate awareness of risks.
Sta surveys: individual
returns and analysis.
1 year after
return.
Review and destroy if no
longer required.
Forms are anonymous so do not contain PID unless
provided in free text boxes. May be required again
ifanalysis is reviewed.
Sta surveys: final report. 10 years. Review and consider transfer
to PoD.
Organisations may want to keep final reports for longer
than the raw data and analysis, for trend analysis over
time. This period can be extended, provided there is
justification and organisational approval.
Trust submission forms. 6 years. Review and destroy if no
longer required.
Retention period in accordance with the Limitation
Act1980.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202249
Communications
Record type Retention
period
Disposal action Notes
Intranet site*. 6 years. Review and consider transfer
to PoD.
Patient information leaflets. 6 years. Review and consider transfer
to PoD.
These do not need to be leaflets from every part of the
organisation. A central copy can be kept for potential
transfer.
Press releases and important
internal communications.
6 years. Review and consider transfer
to PoD.
Press releases may form part of a significant part of the
public record of an organisation which may need to
beretained.
Public consultations. 5 years. Review and consider transfer
to PoD.
Whilst these have a shorter retention period,
theremay be wider public interest in the outcome of
the consultation, particularly where this resulted in
changes tothe services provided, and so may have
historicalvalue.
Website*. 6 years. Review and consider transfer
to PoD.
The PoD may be able to receive these by a regular crawl.
Consult with the PoD on how to manage the process.
Websites are complex objects, but crawls can be made
more eective if certain steps are taken.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202250
Sta records and occupational health
Record type Retention
period
Disposal action Notes
Duty roster. 6 years. Review and if no longer
needed destroy.
Retention begins from the close of the financial year.
Exposure monitoring
information.
40 years or
5years from
the date of the
last entry made
in it.
Review and if no longer
needed destroy.
A. Where the record is representative of the personal
exposures of identifiable employees, for at least
40years or;
B. In any other case, for at least 5 years.
Occupational health reports. Keep until
75th birthday
or 6 years
after the sta
member leaves
whichever is
sooner.
Review and if no longer
needed destroy.
Occupational health report
of sta member under health
surveillance.
Keep until
75thbirthday.
Review and if no longer
needed destroy.
Occupational health report
of sta member under health
surveillance where they have
been subject to radiation
doses.
50 years
from the date
of the last
entry or until
75thbirthday,
whichever is
longer.
Review and if no longer
needed destroy.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202251
Record type Retention
period
Disposal action Notes
Sta record. Keep until
75thbirthday
(see notes).
Review, and consider
transfer to PoD.
This includes, but is not limited to, evidence of right to
work, security checks and recruitment documentation
for the successful candidate including job adverts and
application forms. Some PoDs accession NHS sta
records for social history purposes. Check with your
local PoD about possible accession. If the PoD does
not accession them, then the records can be securely
destroyed once the retention period has been reached.
Sta record: summary. 75th Birthday. Review, and consider
transfer to PoD.
Please see the good practice box sta record summary
used by an organisation. Some organisations create
summaries after a period of time since the sta member
left (usually 6 years). This practice is ok to continue if this
is what currently occurs. The summary, however, needs
to be kept until the sta member’s 75th birthday, and then
consider transferring to PoD. If the PoD does not require
them, then they can be securely destroyed at this point.
Timesheets (original record). 2 years. Review and if no longer
needed destroy.
Retention begins from creation.
Sta training records. See notes. Review and consider transfer
to a PoD.
Records of significant training must be kept until
75thbirthday or 6 years after the sta member leaves.
It can be dicult to categorise sta training records as
significant as this can depend upon the sta member’s
role. The following is recommended: Clinical training
records – to be retained until 75th birthday or six years
after the sta member leaves, whichever is the longer.
Statutory and mandatory training records – to be kept for
ten years after training completed.
Other training records – keep for six years after training
completed.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202252
Record type Retention
period
Disposal action Notes
Disciplinary records. Retain for
6years.
Review and destroy if no
longer required.
Retention begins once the case is heard and any appeal
process completed. The record may be retained for
longer, but this will be a local decision based on the facts
of the case. The more serious the case, the more likely it
will attract a longer retention period. Likewise, a one-o
incident may need to only be kept for the minimum time
stated. This applies to all cases, regardless of format.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202253
Procurement
Record type Retention
period
Disposal action Notes
Contracts sealed or
unsealed.
Retain for
6years after
the end of the
contract.
Review and if no longer
needed destroy.
Contracts – financial
approval files.
Retain for
15years after
the end of the
contract.
Review and if no longer
needed destroy.
Contracts – financial
approved suppliers
documentation.
Retain for
11years after
the end of the
contract.
Review and if no longer
needed destroy.
Tenders (successful). Retain for
6years after
the end of the
contract.
Review and if no longer
needed destroy.
Tenders (unsuccessful). Retain for
6years after
the end of the
contract.
Review and if no longer
needed destroy.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202254
Estates
Record type Retention
period
Disposal action Notes
Building plans,
includingrecords of major
building works.
Lifetime
(ordisposal) of
building plus
6years.
Review and consider transfer
to PoD.
Building plans and records of works are potentially of
historical interest and where possible, should be kept
andtransferred to the local PoD.
Closed circuit television
(CCTV).
Refer to ICO
Code of
Practice.
Review and destroy if no
longer required.
The length of retention must be determined by
the purpose for which the CCTV has been used.
CCTVfootage must remain viewable for the length of
time it is retained, and where possible, systems should
have redaction or censoring functionality to be able to
blank out the faces of people who are captured by the
CCTV, but not subject to the access request, for example,
police reviewing CCTV as part of an investigation.
Equipment monitoring,
andtesting and maintenance
work where ASBESTOS is
afactor.
40 years. Review and destroy if no
longer required.
Retention begins from the completion of the monitoring
ortesting.
This includes records of air monitoring and health records
relating to asbestos exposure, as required by the Control
of Asbestos Regulations 2012.
Equipment monitoring:
general testing and
maintenance work.
Lifetime of
installation.
Review and destroy if no
longer required.
Retention begins from the completion of the testing
andmaintenance.
Inspection reports. Lifetime of
installation.
Review and dispose of if no
longer required.
Retention begins at the END of the installation period.
Building inspection records need to comply with
the Construction (Design and Management)
Regulations2015.
Leases. 12 years. Review and destroy if no
longer required.
Retention begins at point of lease termination.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202255
Record type Retention
period
Disposal action Notes
Minor building works. 6 years. Review and destroy if no
longer required.
Retention begins at the point of WORKS COMPLETION.
Photographic collections:
service locations,
eventsandactivities.
Up to 20 years. Review and consider transfer
to PoD.
These provide a visual historical legacy of the running
and operation of an organisation. They may also provide
secondary uses, such as use in public inquiries.
Radioactive records. 30 years. Review and destroy if no
longer required.
Retention begins at the CREATION of the waste.
If a person handling radioactive waste is exposed to
radiation (accidental or otherwise), then the records
relating to that person must be kept until they reach
75years of age or would have attained that age. In any
event, records must be kept for at least 30 years from the
date of dosing or accident. This also includes patients or
service users who require medical exposure to radiation,
as required by the Ionising Radiation Regulations 2017.
Sterilix Endoscopic
Disinfector Daily Water
CycleTest, Purge Test,
Ninhyndrin Test.
11 years. Review and destroy if no
longer required.
Retention begins from the DATE OF TEST.
Surveys: building or
installation, not patient
surveys.
Lifetime of
installation or
building.
Review and consider transfer
to PoD.
Retention period begins at the END of INSTALLATION
period.
See Inspection reports for legal basis for these records.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202256
Finance
Record type Retention
period
Disposal action Notes
Accounts. 3 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate. Includes all associated documentation
and records for the purpose of audit.
Benefactions. 8 years. Review and consider transfer
to PoD.
These may already be in the financial accounts and
may be captured in other reports, records or committee
papers. Benefactions, endowments, trust fund or legacies
should be oered to the local PoD.
Debtors’ records:
CLEARED.
2 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
Debtors’ records:
NOTCLEARED.
6 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
Donations. 6 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
Expenses. 6 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
Final annual accounts
report*.
Up to 20 years. Review and transfer to PoD. These should be transferred when practically possible,
after being retained locally for a minimum of 6 years.
Ideally, these will be transferred with board papers for
that year to keep a complete set of governance papers.
Financial transaction records. 6 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
Invoices. 6 years from
end of the
financial year
they relate to.
Review and destroy if no
longer required.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202257
Record type Retention
period
Disposal action Notes
Petty cash. 2 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
Private Finance Initiatives
(PFI) files.
Lifetime of PFI. Review and consider transfer
to PoD.
Retention begins at the END of the PFI agreement.
Thisapplies to the key papers only in the PFI.
Sta salary information
orfiles.
10 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
Superannuation records. 10 years. Review and destroy if no
longer required.
Retention begins at the CLOSE of the financial year to
which they relate.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202258
Legal, complaints and information rights
Record type Retention
period
Disposal action Notes
Complaints: case files. 10 years. Review and destroy if no
longer required.
Retention begins at the CLOSURE of the complaint.
The complaint is not closed until all processes
(includingpotential and actual litigation) have ended.
The detailed complaint file must be kept separately from
the patient file (if the complaint is raised by a patient or
in relation to). Complaints files must always be separate.
(Also refer to Appendix III – complaints records).
Fraud: case files. 6 years. Review and destroy if no
longer required.
Retention begins at the CLOSURE of the case. This also
includes cases that are both proven and unproven.
Freedom of Information
(FOI) requests, responses to
the request and associated
correspondence.
3 years. Review and destroy if no
longer required.
Retention begins from the CLOSURE of the FOI request.
Where redactions have been made, it is important to
keep a copy of the response and send to the requestor.
In all cases, a log must be kept of requests and the
response sent.
FOI requests: where there
has been an appeal.
6 years. Review and destroy if no
longer required.
Retention begins from the CLOSURE of the appeal
process.
Industrial relations: including
tribunal case records.
10 years. Review and consider transfer
to PoD.
Retention begins at the CLOSE of the financial year to
which it relates. Some organisations may record these
as part of the sta record, but in most cases, they should
form a distinctive separate record (like complaints files).
Litigation records. 10 years. Review and consider transfer
to PoD.
Retention begins at the CLOSURE of the case.
Litigationcases of significant or major issues (or with
significant, major outcomes) should be considered
for transfer. Minorcases should not be considered for
transfer. If in doubt, consult with the PoD.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202259
Record type Retention
period
Disposal action Notes
Intel patents, trademarks,
copyright, IP.
Lifetime
of patent,
or6years from
end of licence
or action.
Review and consider transfer
to PoD.
Retention begins at the END of lifetime or patent,
orTERMINATION of licence or action.
Software licences. Lifetime of
software.
Review and destroy if no
longer required.
Retention begins at the END of lifetime of software.
Subject Access Requests
(SAR), response,
and subsequent
correspondence.
3 years. Review and destroy if no
longer required.
Retention begins at the CLOSURE of the SAR.
SAR: where there has been
an appeal.
6 years. Review and destroy if no
longer required.
Retention begins at CLOSURE of appeal.

RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
60
Appendix III:
How to de with specific
tpes of records
This appendix provides detailed advice on
records management relating to specific types
of records for example, transgender records,
witnessprotection records and adopted persons
records. These are presented in alphabetical
order. It also provides advice on managing certain
formats of records, for example, emails,
cloud-based records and scanned records.
Adopted persons health records
Notwithstanding any other centrally issued
guidance by the Department of Health, the Welsh
Government and Social Care Wales, the records
of adopted persons can only be placed under the
new last name when an adoption order has been
granted. Before an adoption order is granted,
analias may be used but more commonly the
birthnames are used.
Depending on the circumstances of the adoption
there may be a need to protect from disclosure
any information about a third party. Additional
checks before any disclosure of adoption
documentation are recommended because of the
heightened risk of accidental disclosure.
It is important that any new records, if created,
contain sucient information to allow for a
continuity of care. At present the GP would
initiate any change of NHS number or identity if
itwere considered appropriate to do so following
theadoption.
Ambulance service records
Ambulance service records will contain evidence
of clinical interventions delivered and are
therefore clinical records. This means that they
must be retained for the same time as other
acute or mental health clinical records depending
on where the person is taken to for treatment.
Where ambulance service records are not clinical
in nature, they must be kept as administrative
records. There is a distinction between records
of patient transport and records of clinical
intervention. If the ambulance clinical record is
handed over to another service or NHS trust,
there must be a means by which the ambulance
trust can obtain them again if necessary.
Alternatively, they can be copied and only the
copy transferred, providing this is legible.
Asylum seeker records
Records for asylum seekers must be treated
in exactly the same way as other care records,
allowing for clinical continuity and evidence
of professional conduct. Organisations may
decide togive asylum seekers patient or service
user-hold records (section below) or hold them
themselves. Patient or service user held records
should be subject to a risk assessment because
the record legally belongs to the organisation,
and if required, they must be able to get it back.
There is a risk that patient or service user held
records could be tampered with or altered in an
unauthorised way so careful consideration needs
to be given to this decision.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
61
Audio and visual records
Audio and visual records can take many forms
such as using a dictaphone (digital or analogue)
to record a session or conducting a health or care
interaction using videoconferencing technologies.
The following needs considering when patient or
service user interactions are captured in this way:
Clinical appropriateness
Organisations should decide when it is
appropriate to use audio or visual methods
for the provision of health or care. This should
be documented in organisational policies and
understood by the relevant health and care
professionals.
Retention
If the recording is going to be kept elsewhere
(forexample, as part of the health and care record)
then there is no reason to keep the original
recording provided the version in the main record
is the same as the original or there is a summary
into words which is accurate and adequate for
its purpose. If the recording is the only version or
instance of the interaction, then it must be kept for
the relevant retention period outlined in this Code
(for example, adult, child health or mental health
retention periods). Some recordings may have
archival value (although this is unlikely), and this
should be considered on a case-by-case basis.
Digital continuity
You must consider the medium on which the
recording is made and ensure that it is available
throughout its retention period (for example,
ifthe system or file format is becoming obsolete,
then you will need to migrate it to a newer
platform or format to ensure availability). If it is
a digital recording and you are looking to store
it in the health and care record, ensure the
transfer process captures the authenticity of the
recordingkept.
Storage
Ensure your recordings are stored on systems
you control or are provided to you under contract.
If stored with the product provider, youmust
give them (as controller) clear instructions on
the storage and retention of those images
(forexample, delete one month after the date of
the recording because it has been summarised
into the main health and care record, or retain
for 8 years from consultation with the patient or
service user, then destroy). Providers acting under
contract to a controller are obliged to carry out
their written instruction.
Transparency
You must be transparent with patients and service
users regarding the use of audio and visual
technology, and associated records, so that they
have a reasonable understanding of how they
will be used, why, and what will happen with
the recording after the interaction. For example,
it would be unfair to tell participants that the
recordings are deleted if they are not.
Child school health records
Similar to family records, each child should have
their own school health record rather than a
record for the school (with consecutive entries)
or per year intake. If a child transfers to a school
under a dierent local authority, then the record
will also need to be transferred to the new school
health service provider. This must only be done
once it is confirmed the child is now resident in
the new location. The record must be transferred
securely. The recipient of the record should
contact the sender to confirm receiving the record
(if appropriate). If the records are kept on school
premises, then access must be restricted to health
sta delivering care or other sta who have a
legitimate reason to access them.
Local organisations may operate a paper or digital
system. Records from other child health teams,
following a referral, must be accepted by the
receiving organisation regardless of format.
This is due to safeguarding risks.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
62
Complaints records
Where a patient or service user complains about
a service, it is necessary to keep a separate
file relating to the complaint and subsequent
investigation. Detailed complaint information
should never be recorded in the health and care
record. A complaint may be unfounded or involve
third parties and the inclusion of that information
in the health or care record will mean that the
information will be preserved for the life of the
record and could cause detrimental prejudice to
the relationship between the patient or service
user and the health and care team. In some cases,
it may be appropriate to share details of the
complaint with the health and care professional
involved in providing individual care in order to
make improvements in care delivery. However,
there may also be times where the complaint is
about an individual but not care related and it
might not be appropriate to share details of the
complaint with that person, in case further action
is required. The complaints team should review
each complaint on a case-by-case basis.
Where multiple teams are involved in the
complaint handling, all the associated records
must be brought together to form a single record.
This will prevent the situation where one part of
the organisation does not know what the other
has done. A complaint cannot be fully investigated
if the investigation is based on incomplete
information. It is common for the patient or service
user to ask to see a copy of their complaint file
and it will be easier to deal with if all the relevant
material is in one file. Where complaints are
referred to the Ombudsman Service, a single file
will be easier to refer to.
Health and care organisations should have a
local policy to follow with regards to complaints,
covering how information will be used once
any complaint is raised, and after the complaint
has been investigated, regardless of outcome.
TheICO has also issued guidance on complaints
files and who can have access to them, which will
drive what must be stored in them.
Contract change records
Once a contract ends, any service provider still
has a liability for the work they have done and,
as a general rule, at any change of contract the
records must be retained until the time period
forliability has expired.
In the standard NHS Standard contract
(Wales) 2006 there is an option to allow the
commissioner to direct a transfer of care records
to a new provider for continuity of service and
this includes third parties and those working
under any qualified provider contracts. This will
usually be to ensure the continuity of service
provision (forcurrent cases) upon termination
of the contract. Itis also the case that after the
contract period has ended, the previous provider
will remain liable for their work. In this instance
there may be a need to make the records
available for continuity of care or for professional
conductcases.
When a service is taken over by a new
provider, the records of the service (current and
discharged cases) all transfer to the new provider
(unlessdirected otherwise by the commissioner
of the service). This is to ensure that the records
for the service remain complete and enable
patients or service users to obtain their record if
they so request it. It also makes the records easier
to locate if they are required for other purposes.
This will also stop the fragmentation of the archive
records for the service and make it much easier
toretrieve records.
Where legislation creates or disbands public
sector organisations, the legislation will normally
specify which organisation holds liability for
any action conducted by a former organisation.
Thismay also include consideration of the
identity of the legal entity, which must manage
therecords.
In some cases, records may end up orphaned.
This may happen where the organisation that
created them is being disbanded and there is no
successor organisation to take over the service or
provision.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
63
In these cases, orphaned records need to be
retained by the highest level commissioner of that
service or provision. Forexample, if a GP practice
closes, patients will be oered the choice to
register with another nearby practice. Whenthey
register with the new practice, therecord will
follow the patient to that new practice. However,
if a practice closes, and the patient does not
re-register elsewhere, the record will transfer to
Primary Care Services within NHS Wales Shared
Services Partnership.
Where the content of records is confidential,
for example, health and care records, it will be
necessary to inform the individuals concerned
about the change. Where there is little impact
upon those receiving care, it may be sucient to
use posters and leaflets to inform people about
the change, but more significant changes will
require individual communications. Although the
conditions of UK GDPR may be satisfied, in many
cases there is still a duty of confidentiality which
may require a patient or service user (in some
cases) to agree to the transfer, dependent upon
the legal basis and the implications of their choice
discussed with them. If the new provider has a
statutory duty to provide the service, then consent
does not need to be sought. If there is no statutory
duty, then consent would need to be sought to
satisfy the common law duty of confidentiality.
It is vital to highlight the importance of actively
managing records, which are stored in osite
storage (refer to section three of the Code for
further information on osite storage including
theimportance of completing a DPIA).
These principles and guidance can also apply
to non-clinical situations as well, such as when
LocalHealth Boards (LHBs) merge or a trust takes
over the running of another one.
Annex 1 of this appendix summarises the
considerations and actions required relating
tovarious contract change situations.
Continuing healthcare (CHC) records
Continuing healthcare records can be split into
two parts:
Care record
The care record is the information relating to
a patient or service user’s care that enables
the CHC panel to determine eligibility for CHC
based on an assessment of needs. This can be
provided directly by the patient or service user or
obtained from health and care providers as part
of the eligibility process. Consent to obtain this
information would be required to satisfy the duty
of confidence. The initial checklist completed
by the referrer may also contain some level of
confidential information and this may also be used
to determine eligibility.
Administrative record
The administrative record is the information used
by the LHB to ensure the CHC process runs
eectively – an example being appointment
letters asking the patient or service user to
attend a panel. LHBs require access to health
and care information to determine a patient or
service user’s entitlement (once the LHB has
beennotified).
CHC records should be kept for the same
period of time as adult and child health records,
fromthe date the case is decided by the CHC
panel. Where CHC cases relate to mental health,
theseshould be kept for the same period of time
as mental health records.
Controlled drugs regime
NHS Wales, in conjunction with the NWSSP
and their PCS, has established procedures
for handling information relating to controlled
drugs. Thisguidance includes conditions for
storage, retention and destruction of information.
Whereinformation about controlled drugs is
held please refer to TheControlled Drugs
(Supervisionof Management and Use) (Wales)
Regulations 2008.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
64
Duplicate records
The person or team to which the record relates
will normally hold the original record however
occasionally duplicates may be created for
legitimate business purposes. It is not necessary
to keep duplicates of the same record unless it
is used in another process and is then a part of a
new record. Where this is not required, the original
should be kept, and the duplicate destroyed.
Forexample, incident forms, once the data is
entered into the risk information system, the paper
is now a duplicate, and so can be destroyed.
Some clinical systems allow printouts of digital
records. Where printouts are used, these must be
marked as duplicates or copies to help prevent
them from being used as the primary record.
Evidence required for courts
In UK Law, the civil procedure rules allow
evidence to be prepared for court and, aspart
of this, theparties in litigation can agree what
documents they will disclose to the other
party and, ifrequired, dispute authenticity.
Thedisclosure of digital records is referred to as
E-Disclosure or E-Discovery. The relevant part for
disclosure and admissibility of evidence is given
in the Ministry of Justice’s Civil Procedure Rules–
Part31. Ifrecords are arranged in an organised
filing system, such as a business classification
scheme, or all the relevant information is placed
on the patient or client file, providing records as
evidence will be much easier. Further advice on
electronic records and evidential weighting can
be found in BIP10008: Evidential Weight and
Admissibility ofElectronic Information.
Family records
Family records used to be common within
health visiting teams, amongst others, where a
whole family view was needed to deliver care.
Whilstthese records should no longer be created,
theyare included here for legacy reasons.
Due to changes in the law and best practice, it is
not advisable to create a single paper or digital
record that contains the care given to all family
members. Each person is entitled to privacy and
confidentiality, and having all a person’s records
inone place could result in a health professional
or family member accessing confidential
information of another family member accidentally
or otherwise.
Good practice would be to create an individual
file for each person but with cross references
to other family members. This means that each
individual has their own record, but health and
care professionals can see who else is related
to that person, and so can check these records
where necessary. Single records also help to
protect privacy and confidentiality and (if digital)
keep anaudit trail of access.
General Practitioner records
It is important to note that the General Practitioner
(GP) record, usually held by the General Practice,
is the primary record of care and the majority
of other services must inform the GP through a
discharge note or a clinical correspondence that
the patient has received care. This record is to
be retained for the life of the patient plus at least
ten years after death. The GP record transfers
with the individual as they change GP throughout
their lifetime. Where the patient has de-registered,
records should be kept for 100 years since
de-registration. A review is taking place to
ascertain how long this period should be in the
going forwards.
Current guidance advises that the content of
paper Lloyd George records should only be
destroyed once they have been scanned to
the required standard and quality assurance
of the scanned images has been completed,
confirmingthat they are a like for like copy of
the original paper records. The Lloyd George
envelope itself should not be destroyed at the
current time and must be kept to meet with
the requirements for patient record movement.
Further Advice from PCS can be found in the
Practice Guidance Notes for Registration Links.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
65
Individual funding requests (IFRs)
Similar to CHC, IFR cases are mainly administrative
records, but also contain large amounts of
personal or confidential patient information and
as such, should be treated in the same way as
CHCrecords.
As IFRs are unique to an individual, it may be that
the care package given to the patient or service
user is unique and bespoke to that person.
Thiscould mean that the record may have
long-term archival value, due to the uniqueness
of the care given in this way, and so potentially
may be of interest to The National Archives.
Local discussions should be held with the PoD to
determine the level of local interest, althoughthey
would not normally get involved at this level of
discussion. It would be a joint discussion on the
principle and agreement to archive this type of
record and then the responsibility of the health
and care organisation to choose individual records
that meet this criteria.
Integrated records
Since 2013, there has been an increase in the
number of initiatives promoted and launched that
involve integrated records. There has also been
recognition nationally that joined up delivery
of health and care services can increase the
quality of care delivered, and also deliver those
services more eciently. The vision and strategy
in the following documents shows the vision for
integrated care records in Wales:
• A Healthier Wales;
• Well-being of Future Generations Act.
Depending on the agreements under which
integrated records are established these may be
subject to the Public Records Act. Generally, ifan
NHS Wales body is at least partly responsible
for the creation and control of the record, it will
normally be considered a public record to be
managed in accordance with the Act. The relevant
PoD should be notified that this is the case. If in
doubt, consult with The Archives.
The options for organisations will depend on what
local architecture and systems are already in use.
There are three types of retention for integrated
records, and suggested retention periods foreach.
1. All organisations contribute to a single record,
creating the only record for that patient or
service user. Consideration must be given to
how this is managed in practice (for example,
some records will be retained for 8 years and
some for 20 years but they will look the same
at face value) (retain for the longest specialty
period involved).
2. All organisations pool their records into a single
place but keep a level of separation between
each type of record (retain for each specialty
asapplicable – because they are not merged).
3. All organisations keep their own records, but
allow others to view their records, but not
amend or add to (retain for each specialty as
applicable – because they are not merged).
Where organisations are looking to create
integrated records, they must enter into a joint
controller arrangement, which detail the purpose
and method of integrated records. It should also
set out how disputes between controllers may
be resolved. Information materials for patient or
service users must also reflect how their records
are used.
Increasingly, where organisations are using
this type of system, the information contained
within has the potential to be used for purposes
other than individual care, such as Population
Health Management (PHM). PHM is a tool that is
increasingly being used to help plan and prepare
care provision in a particular geographical area or
specialty. Where this is proposed, controllersmust
assure themselves of the lawfulness of any
proposed new usage under UK GDPR and Duty
of Confidence. See also the section on integrated
viewing technology and record keeping in the
format section below.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
66
Occupational health (OH) records
Occupational health records are not part of the
main sta record and for reasons of confidentiality
they are held separately. It is permitted for
reports or summaries to be held in the main sta
record where these have been requested by
the employer and agreed by the sta member.
Whenoccupational health records are outsourced,
the organisation must ensure that:
• sta are aware of the outsourcing and how
their information may be used for OH purposes;
• the contractor can comply as necessary
with data protection and confidentiality
requirements;
• there is a contract in place with the outsourced
provider that has legally binding clauses in
relation to data protection and confidentiality;
• the contractor can retain records for the
necessary period after the termination of
contract for purposes of adequately recording
any work-based health issues and is able to
present them to the organisation if required.
Pandemic records
Health and care organisations will create records
as part of a response to a global pandemic.
Pandemic events are rare but will nevertheless
create records that need to be managed.
Both patient and service user records will be
created that detail the care given to people
aected by the pandemic. Corporate records will
also be created which record business decisions,
policies and processes that were taken in
response to a pandemic.
These records should be managed in accordance
with the retention schedules set out in this Code.
Organisations should be mindful that a public
inquiry (or inquiries) is likely to take place after a
pandemic so the pandemic related records could
be used or requested as part of that Inquiry.
TheUK Government has already agreed to hold
apublic inquiry into the coronavirus pandemic that
began in 2020.
If organisations have created records specifically
in response to a pandemic, these should not be
destroyed when they have reached their minimum
retention period, unless the public inquiry has
ended, or the Inquiry has provided guidance
on what type of records it will be interested
in. Thesespecific records may have historical
value, so discussions should take place with your
local PoD. A policy on how to manage a new
admission to a care home of an individual with
acoronavirus diagnosis may be of interest to the
PoD, whereasthe care record might not have the
same value and should be managed as a health
and care record. Any guidance or advice issued
by National Archives Wales or your local PoD in
relation to the preservation of pandemic records
should be followed.
Patient or service user held records
Some clinical or care services may benefit from
the patient or service user holding their own
record, for example, maternity services. Where this
is considered to be the case a risk assessment
should be carried out by the organisation. Whereit
is decided to leave records with the individual
who is the subject of care, it must be indicated on
the records that they remain the property of the
issuing organisation and include a return address
if they are lost. Upon the discharge of the patient
or service user, the record must be returned to
the health or care organisation involved in the
person’s care.
Organisations must be able to produce a record
of their work, which includes services delivered
inthe home where the individual holds the record.
Upon the termination of treatment, where the
records are the sole evidence of the course of
treatment or care, they must be recovered and
given back to the issuing organisation.
A copy can be provided if the individual wishes
to retain a copy of the records through the SAR
process. In cases where the individual retains the
actual record after care, the organisation must be
satisfied it has a record of the contents.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
67
Patient or service user portals
Organisations may implement products that
provide patients and service users with access
totheir records. Access may be either online or
via an app or portal. There are increasing numbers
of commercial organisations that are providing
theseproducts.
The provision of these products must comply
with data protection legislation, and other
relevant laws such as the Common Law Duty of
Confidentiality. Health and care organisations
must conduct a DPIA if they are considering using
such a product. Health and care organisations
must remain controller for the patient or service
user’s information. In most cases, the supplier of
the product or system will be a processor as the
product facilitates access to the information held
by health and care organisations.
Controllers must consider what is relevant and
proportionate to include in this type of record.
Some information may not be appropriate to add
to the portal, for example, harmful information
a patient does not know yet because the
intention is to let them know in person during
aconsultation.
Information about the patient or service user
must not be uploaded into the product until there
is a clear legal basis for doing so, for example,
patient consent. Individuals must be provided
with information materials so that they can make
an informed choice as to whether or not to sign
up. The materials should also make it clear what
information patients and service users can upload
themselves directly to the portal if this is an option.
It should also be clear to the patient or service
user who controls the information.
Information stored in a product like this should
be retained in line with the retention schedules
outlined in this Code (for example, adult health
records for 8 years after last seen).
Pharmacy held patient records
These are the records of patients that the
pharmacy has dispensed medications to or
had some other form of clinical interaction with
(forexample, given a flu jab) – similar to a hospital
or care home patient record.
Records of prescriptions dispensed will be kept
by NWSSP and their PCS so there is no need to
keep a copy of the prescription locally except for
auditpurposes.
Other elements of the pharmacy record,
forexample, vaccinations provided, should be
viewed in the same way as a patient record,
and should be destroyed 8 years after the last
interaction with the patient. However, if there is
aneed to keep the record for longer, then this
canbe extended up to 20 years, provided there
isa justified, documented and approved reasons
for doing so. Information materials for patients
should also be reflective of the organisation’s
retention period.
Prison health records
Responsibility for oender health in HM Prison
Services in Wales is held by local Health Boards.
A national computer-based record created by the
Ministry of Justice was created to facilitate the
provision of care and the transfer of care records
associated with inmate transfers throughout
imprisonment. Digital Health and Care Wales
(DHCW) have been helping Health Boards to
facilitate the use of this system in Wales.
A significant number of paper records remain,
and some oender health services operate a
mix of paper and digital records. Prison records
should be treated as hospital episodes and may
be disposed of after the appropriate retention has
been applied. The assumption is that a discharge
note has been sent to the GP.
Where a patient or service user is sent to prison
the GP record (or social care record) must not be
destroyed but held until the patient is released
ornormal retention periods of records have
beenmet.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
68
Prison health records may have archival value,
but this is the exception rather than rule.
Recordsshould be kept in line with the same
period as for de-registered GP records, witha
view to further retention (with justification)
and a potential transfer to a PoD, subject to
theirapproval.
Private patients treated on NHS
Walespremises
Where records of individuals who are not
NHSWales or social care funded are held in the
record keeping systems of NHS Wales or social
care organisations, they must be kept for the
same minimum retention periods as other records
outlined in this Code. The same levels of security
and confidentiality will also apply.
Public health records
A local authority normally hosts public health
functions, but the functions still involve the
handling of health and care information. Forthis
reason, public health functions are in the scope
of this Code. Where clinical information is
being processed by the public health function
it is expected to comply with the Code of
Confidentiality for Health and Social Care in
Wales(2005).
Records relating to sexually
transmitteddiseases
Organisations that provide care and support under
The National Health Service (Venereal Diseases)
Regulations 1974 must be aware of the additional
obligations to confidentiality these impose
on employees and trustees of organisations.
Theseorganisations include NHS Trusts, LHBs,
local authority public health teams and those
providing services under NHS contracts in Wales.
This obligation diers from the duty of
confidentiality generally because it prohibits some
types of sharing but enables sharing where this
supports treatment of patient or service users.
For this reason, it is common for services dealing
with sexually transmitted diseases to partition
their record keeping systems to comply with the
directions and more generally to meet patient
or service users’ expectations that such records
should be treated as particularly sensitive.
Secure units for patients detained under
the Mental Health Act 1983
Mental health units operate on a low, mediumand
high-risk category basis. Not all patients on these
units will have been referred via the criminal
justice system. Some patients may be deemed
a risk under the Mental Health Act and will need
to be accommodated accordingly. Some patients
may be high-risk due to the nature of a crime they
have committed because of their mental health
and therefore will need to be accommodated
accordingly. As such, their records should be
treated in the same way as other mental health
records including retention periods (20 years,
andlonger if justified and permitted) and final
disposal. A long retention time may also help sta
at these units deal with subsequent long-term
enquiries from care providers.
Sexual assault referral centres
Sexual assault referral centres (SARCs) are
highly specialised forensic and health services
co-commissioned by Police and Crime
Commissioners and Local Health Boards.
SARCs support the physical, mental health and
wellbeing of service users and collect forensic
evidence pertaining to alleged sexual oences.
Records generated may include forensic medical
examination notes, body maps, photographic
records, and DNA intelligence. Reports or
statements on these records may be required
as evidence in a court of law, and the records
management process must facilitate this.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
69
Basedon relevant guidance, legal and regulatory
obligations, a minimum retention period of
30years for SARC records has been applied
by NHS Wales This retention period reflects the
severity of the alleged oence; the length of
time for the potential bringing of criminal justice
proceedings and right to appeal; and the potential
for cold case review. Retaining records beyond
30 years is acceptable provided there is ongoing
justification and the decision is documented and
approved by the relevant committees responsible
for the SARCs operational delivery.
Specimens and samples
The retention of human material is covered by
this Code because some specialities will include
physical human material as part of the patient or
service user record (or linked to it). The record
may have to be retained longer than the sample
because the sample may deteriorate over
time. Relevant professional bodies such as the
Human Tissue Authority or the Royal College
of Pathologists have issued guidance on how
long to keep human material. Physical specimens
or samples are unlikely to have historical value,
andso are highly unlikely to be selected for
permanent preservation.
The human material may not be kept for long
periods, but that does not mean that the
information or metadata about the specimen
orsample must be destroyed at the same time.
The information about any process involving
human material must be kept for continuity of
care and legal obligations. The correct place to
keep information about the patient is the clinical
record and although the individual pathology
departments may retain pathology reports, a copy
must always be included on the patient record.
Physical specimens or samples do not have to be
stored within the clinical record (unlessdesigned
to do so) but can be stored where clinically
appropriate to keep the material, with a clear
reference or link in the clinical file, so both the
material and the clinical record can be joined
together if necessary.
Sta records
Sta records should hold sucient information
about a sta member for decisions to be made
about employment matters. The nucleus of any
sta file will be the information collected through
the recruitment process and this will include
the job advert, application form, evidence of
the right to work in the UK, identity checks and
any correspondence relating to acceptance of
the contract. The central HR file must be the
repository for this information, regardless of the
media of the record.
It is common practice in some health and care
organisations for the line manager to hold a
truncated record, which contains portions of
an employee’s employment history. This can
introduce risk to personal information (as it
is duplicated), but also potentially expedient
to do so. Organisations considering whether
to use, ordiscontinue using, local HR files,
shouldcomplete a risk assessment.
Information kept in truncated sta files should be
duplicates of the original held in the central HR file.
If local managers are given originals as evidence
(such as a sta member bringing in a certificate
of competence) they should take a copy for local
use and the original should be kept with the
main HRfile. It is important that there is a single,
complete employment record held centrally for
reference and probity.
Upon termination of contract (for whatever
reason), records must be held up to and beyond
the statutory retirement age. Sta records may
be retained beyond 20 years if they continue
to be required for NHS Wales or organisational
business purposes, in accordance with Retention
Instrument122. Usually this relates to inpatient
ward areas, where the ward manager will keep
a small file relating to the training and clinical
competencies of ward sta. Where there is
justification for long retention periods or protection
is provided by the Code, this will not be in breach
of GDPRPrinciple5. (Refer to Section 5 of the
Code for further information about retention
ofrecords).
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
70
Some organisations operate a weeding system,
whereby sta files are culled of individual
record types that are now time expired (such as
timesheets). Others have just kept the whole file
as is and archived it away until 75th birthday. It is
not recommended to change your system from
one to the other because:
• the eort involved would be disproportionate
to the end result;
• if you begin to weed files, you would need
to do this retrospectively to all files, to avoid
having two types of central HR file;
• you cannot reverse the weeding process
– ifyou decide to keep full records, it is
impossible to remake historically weeded files
complete again.
Both systems are acceptable, regardless of media.
It is noted that organisations may have a hybrid
system of paper historical sta files and digital
current sta files. If possible, organisations should
consider moving all their files into one format to
create consistency.
Where an organisation decides to use a summary,
it must contain as a minimum:
• a summary of the employment history
withdates;
• pension information including eligibility;
• any work-related injury;
• any exposure to asbestos, radiation and other
chemicals which may cause illness in later life;
• professional training history and professional
qualifications related to the delivery of care;
• list of buildings where the member of sta
worked, and the dates worked in each location.
Disciplinary case files should be held in a separate
file so they can be expired at the appropriate
time and do not clutter up the main file. Thatdoes
not mean that there should be no record that
the disciplinary process has been engaged in
the main record, as it may be pertinent to have
an indication to the disciplinary case, but the full
details and file must be kept separately from the
main file.
With regards to sta training records, it can be
dicult to categorise them to determine retention
requirements but keeping all the records for the
same length of time is also hard to justify. It is
recommended that:
• clinical training records are retained until
75thbirthday or six years after the sta
member leaves, whichever is the longer;
• statutory and mandatory training records are
kept for ten years after training is completed;
• other training records are kept for six years
after the training is completed.
The Chartered Institute for Personnel and
Development, and the ICO have provided further
information and advice on the retention of
HRrecords.
Transgender patients’ records
Sometimes patients change their gender and part
of this may include medical care. Recordsrelating
to these patients or service users are often seen
as more sensitive than other types of medical
records. While all health and care records are
subject to confidentiality restrictions, there are
specific controls for information relating to patients
or service users with a Gender Recognition
Certificate. The use and disclosure of the
information contained in these records is subject
to the Gender Recognition Act 2004, (GRA) which
details specific restrictions and controls for these
records. The GRA is clear that it is not an oence
to disclose protected information relating to a
person if that person has agreed to the disclosure.
The GRA is designed to protect transgender
patient and service user data and should not
be considered a barrier to maintaining historic
medical records where this is consented toby
theuser.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
71
Nearly all actions relating to transgender records
will be based on explicit consent. Discussions
will take place between the GP and the patient
regarding clinical care, what information in their
current record can be moved to their new record
and any implications this decision may have
(forexample, they may not be called for a gender
specific screening programme). Patients should be
oered ways to maintain their historical records.
This could include editing previous entries and
removing references containing previous names
and gendered language. Any decisions made
regarding their record must be respected and
therecords actioned accordingly.
Any patient or service user can request that
their gender be changed in a record by a
statutory declaration, but the Gender Recognition
Act2004 provides additional rights for those
with a GRC. The formal legal process (as defined
in the Gender Recognition Act 2004) is that a
Gender Reassignment Panel issues a Gender
Reassignment Certificate. At this time a new
NHSnumber can be issued, and a new record can
be created, if it is the wish of the patient or service
user. It is important to discuss with the patient
or service user what records are moved into the
new record and to discuss how to link any records
held in any other health or care settings with the
new record, including editing previous records
to remove names, gender references or details.
Thecontent of the new record will be based on
explicit consent under common law.
However, it is not essential for a transgender
person to have a GRC in order to change
their name and gender in their patient record
and receive a new NHS number. They do not
need tohave been to a Gender Identity Clinic,
takenanyhormones, undergone any surgery,
orhave a Gender Recognition Certificate.
Under the Equality Act (2010), Transgender
people share the protected characteristic of
“gender reassignment”. To be protected from
gender reassignment discrimination, an individual
does not need to have undergone any specific
treatment or surgery to change from their birth
sex to their preferred gender. This is because
changing physiological or other gender attributes
is a personal process rather than a medical one.
An individual can be at any stage in the transition
process – from proposing to reassign their gender,
to undergoing a process to reassign their gender,
or having completed it.
Protected persons health records
Where a record is that of someone known
to be under a protected person scheme,
therecord must be subject to greater security
and confidentiality. It may become apparent
(viaaccidental disclosure) that the records are
those of a person under the protection of the
courts for the purposes of identity. The right to
anonymity extends to health and care records.
For people under certain types of protection,
theindividual will be given a new name and NHS
Number, so the records may appear to be that of
adierent person.
Welsh and English language records
guidance
Legislation and policy in Wales support the Welsh
language recording on patient and clinical records.
In terms of recording on patient and care clinical
records, the following protocol is advocated as
best practice:
English records:
• When a service user language is English
all the records will be written in English by
both English and Welsh language speaking
practitioners.
• English service user/ English practitioner –
the practitioner writes up the record note
inEnglish.
• English service user/ Welsh practitioner –
the Welsh practitioner would undertake the
consultation in English and the interaction
would be recorded in English (the language
ofthe interaction).
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
72
Bilingual records:
Bilingual records will be required for services
users accessing services in Welsh in the
followingscenarios:
• Welsh service user/Welsh practitioner –
aWelsh speaking service user receives a
consultation in Welsh from a Welsh practitioner.
The practitioner can write up the record
note in English or in Welsh (the language of
the interaction) and arrange for a full English
translation to also be included within the
record. If the service user requests a copy of
the record in Welsh the English record will be
translated and provided bilingually.
• Welsh service user/English practitioner –
ifa Welsh speaking service user receives
a consultation from a practitioner in English
the interaction will be recorded in English
(thelanguage of the interaction). If the
service user request a copy of the record
in Welshtherecord will be translated and
provided bilingually.
Youth oending service records
Due to the nature of youth oending it is common
for very short retention periods to be imposed on
the general youth oending record. Forpurposes
of clinical liability and for continuity of care the
health or social care portion of the record must
be retained as specified in this Code. Thiswill
generally be until the 25th birthday of the
individual concerned.
Format of record:
Bring your own device (BYOD)
createdrecords
Any record that is created in the context of health
and care business is the intellectual property
of the employing organisation and this extends
to information created on personally owned
computers and equipment. This in turn extends
to emails and text messages sent in the course
of business on personally owned devices from
personal accounts. They must be captured in the
record keeping system if they are considered to
fall within the definition of a record.
When an individual sta member no longer works
for the employing organisation, anyinformation
that sta take away could be a risk to the
organisation. If this includes personal data or
confidential patient information, it is reportable
tothe ICO and may be a breach of confidentiality.
For this reason, personal/confidential patient
information should not be stored on the device
unless absolutely necessary and appropriate
security is in place. Local health and care
organisations should have a policy on the use of
BYOD by sta. Also refer to guidance on BYOD.
Cloud-based records
Use of cloud-based solutions for health and
care is increasingly being considered and used
as an alternative to manage large networks
andinfrastructure.
Before any cloud-based solution is implemented
there are a number of records considerations that
must be addressed as set out by The National
Archives. The ICO has issued guidance on cloud
storage. Organisations must complete a DPIA
when considering using cloud solutions.
Another important consideration is that at some
point the service provider or solution will change
and it will be necessary to migrate all of the
records, including all the formats, ontoanother
solution. Whilst this may be technically
challenging, it must be done, and contract
provisions should be in place to do this.
Records in cloud storage must be managed just
as records must be in any other environment and
the temptation to use ever-increasing storage
instead of good records management will not
meet the records management recommendations
of this Code. For example, if digital health and
care records are uploaded to cloud storage for
the duration of their retention period, then they
must contain enough metadata to be able to be
retrieved and a retention date applied so it can
bereviewed and actioned in good time.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
73
Personal data that is stored in the cloud, andthen
left, risks breaching UK GDPR by being kept
longer than necessary. This information would also
be subject to Subject Access process, and if not
found or left unfound, would be a breach of the
patient or service user’s rights.
Email and record keeping implications
Email is widely accepted as the primary
communication tool used every day by all levels
ofsta in organisations. They often contain
business (or in some cases clinical) information
that is not captured elsewhere and so need to be
managed just like other records. NHS Wales and
DHCW have an All Wales Email Use Policy which
should be followed.
Email has the benefit of fixing information in
time and assigning the action to an individual,
whichare two of the most important
characteristics of an authentic record.
However,acommon problem with email is that
itisrarely saved in the business context.
The correct place to store email is in the record
keeping system according to the business
classification scheme or file plan activity to which
it relates. Solutions such as email archiving and
ever-larger mailbox quotas do not encourage
sta to meet the standard of storing email in the
correct business context and to declare the email
as arecord.
Where email archiving solutions are of benefit is as
a backup, or to identify key individuals where their
entire email correspondence can be preserved as
a public record.
Where email is declared as a record or as a
component of a record, the entire email must
be kept, including attachments so the record
remains integral. For example, an email approving
a business case must be saved with the business
case file. All sta need to be adequately trained in
required email storage and organisations need to:
• undertake periodic audits of working practice
to identify poor practice;
• have a policy in place that covers email
management – including the appraisal,
archiving and disposal of emails;
• take remedial action where poor practice
orcompliance is found.
Automatic deletion of email as a business rule
may constitute an oence under Section 77
of the FOIA where it is subject to a request for
information, even if the destruction is by automatic
rule. The courts’ civil procedure rules 31(B)
also require that a legal hold is placed on any
information including email when an organisation
enters into litigation. Legal holds can take many
forms and records cannot be destroyed if there is
a known process or a reasonable expectation that
records will be needed for a future legal process
such as:
• local inquiries into health or care issues;
• national inquiries;
• public inquiries;
• criminal or civil investigations;
• cases where litigation may be reasonably
expected, for example, a patient has indicated
they will take the organisation to court;
• a SAR (known or reasonably expected);
• a FOI request (submitted or reasonably
expected).
This means that no record can be destroyed by
apurely automated process without some form
ofreview whether at aggregated or individual level
for continued retention or transfer to a PoD.
The NADEXID system allows a single email
account for every sta member that can follow
the individual through the course of their career.
Whensta transfer from one NHS organisation
in Wales to another, they must ensure that no
sensitive data relating to the former organisation
istransferred.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
74
It is good practice for sta to purge their email
accounts of information upon transfer to prevent a
breach of confidence or the transfer of classified
information. This is facilitated by sta storing only
emails that need to be retained on anongoing
basis.
Emails that are the sole record of an event or
issue, for example, an exchange between a
clinician and a patient, should be copied into the
relevant health and care record rather than being
kept on the email system or deleted.
Instant messaging records
Health and care services are increasingly using
instant messaging apps or platforms to share
patient and service user information between
health and care professionals or to contact
patients or services users in a transactional way,
such as appointment reminders.
Instant messaging apps or platforms should not
beused as the main, or primary, record for a
person. Where possible, information shared in
this way also needs to have a place in the health
or care record of that person. This could be a
printout of the exchange; contents transcribed into
the record; or a progress note accurately covering
the exchange entered into the record. If the app
or platform is the only place that information
is stored, then it must be managed in line with
thisCode.
Transactional messages, such as GP appointment
reminders or pharmacy notifications that your
prescription is ready for collection, have a short
shelf-life and will no longer be needed once
the appointment is attended or prescriptions
collected. Organisations that use these systems
should keep a record of messages sent to a
person, in case they are needed later (suchas
proof that the patient was reminded of their
appointment), but once it is clear that the purpose
of the message has been fulfilled, there is no
requirement to keep these messages.
Integrated viewing technology and
recordkeeping
Many record keeping systems pool records to
create a view or portal of information, which can
then be used to inform decisions. This in eect
creates a single digital instance of a record,
whichis only correct at the time of viewing.
This may lead to legacy issues, especially in
determining the authenticity of a record at any
given point in the past. When deciding to use
systems that pool records from dierent sources,
organisations must be assured that the system can
recreate a record at a given point in time, andnot
just be able to provide a view at the time of
access. Thiswill enable a health or care provider
to show what information was available at the time
a decision was made.
Consideration should also be given to the
authenticity and veracity of the record,
particularlyif there is conflicting information
presented by two or more contributors to the
record. Some conflicts may be easier to resolve
than others, for example, a person has a dierent
address with two systems), however more
complex conflicts would require organisations
to have a process or procedure to agree how
toresolve these.
Scanned records
This section applies to health and care records
as much as it does to corporate records.
Whenlooking to scan records, organisations need
to consider the following:
• the scanned image can perform equally as well
as the original paper;
• scanned images can be challenged in court
(just as paper can);
• ability to demonstrate authenticity of the
scanned image;
• ensure technical and organisational
measures are in place to protect the integrity,
usabilityand authenticity of the record, over its
period ofuse and retention;
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
75
• discussions need to take place with the local
PoD over records that may be permanently
accessioned – they will need input into the
format of the transferring record;
• where the hard copy is retained, this will be
legally preferable to the scanned image.
The legal admissibility of scanned records, aswith
any digital information, is determined by how
it can be shown that it is an authentic record.
Anindication of how the courts will interpret
evidence can be found in the civil procedure rules
and the court will decide if a record, either paper
or digital, can be admissible as evidence.
The British Standards Institution has published
astandard that specifies the method of ensuring
that electronic information remains authentic.
The standard deals with both “born digital”
and scanned records. The best way to ensure
that records are scanned in accordance with
the standard is to use a supplier or service that
meets the standard following a comprehensive
procurement exercise, which complies with
NHS Wales’ due diligence. Using a BSI10008
accredited supplier, or an in-house accredited
service would be seen as best practice.
For local scanning requirements or for those
records where there is a low risk of being required
to prove their authenticity, organisations may
decide to do their own scanning following due
diligence and internal compliance processes.
Thismay require a business case to be drawn
upand approved, and procurement rules followed
topurchase the necessary equipment.
Once scanned records have been digitised
andthe appropriate quality checks completed,
it will then be possible to destroy the paper
original, unless the format of the original has
historical value, in which case consideration
should be given to keeping it with a view to
permanent transfer. Where paper is disposed of
post-scanning, this decision must be made by the
appropriate group or committee. A scan of not less
than 300 dots per inch (or 118 dots per centimetre)
as a minimum is recommended for most records
although this may drop if clear printed text is being
scanned. Methods used to ensure that scanned
records can be considered authentic are:
• board or committee level approval to
scanrecords;
• a written procedure outlining the process
to scan, quality check and any destruction
process for the paper record;
• evidence that the process has been followed;
• technical evidence to show the scanning
system used was operating correctly at the
time of scanning;
• an audit trail or secure system that can show
that no alterations have been made to the
record after the point they have been digitised;
• fix the scan into a file format that cannot
beedited.
Some common mistakes occur in scanning by:
• only scanning one side and not both
sides, including blank pages – to preserve
authenticity, both sides of the paper record,
even if they are both blank, must be scanned
(this ensures the scanned record is an exact
replica of the paper original);
• scanning a copy of a copy – leading to a
degraded image;
• not using a method that can show that the
scanned record has not been altered after it
has been scanned – questions could be raised
regarding process and authenticity;
• no long-term plan to enable the digitised
records to be stored or accessed over the
period of their retention.
Once you have identified digital records that
are suitable for accessioning to your local
PoD or The National Archives (for national
bodies, itisrecommended to follow published
TheNational Archives guidance on the
accessioning of digital records.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 2022
76
Social media
Organisations must have approved policies and
guidance when using social media platforms.
Itis acknowledged that social media will mainly be
used for promoting activities of the organisation,
rather than as a way of communicating care issues
or interventions with patients or service users.
Information posted on social media may also be
classed as a corporate record and appropriate
retention periods set where applicable.
Information posted on social media (such as
details of upcoming meetings, or published
policies) will usually be captured elsewhere in
an organisation’s corporate records’ function,
and where this is the case, there is no value in
retaining the information held in the social media
platform, as it will be a duplication of the corporate
records management function.
Website as a business record
As people interact with their public services,
more commonly it is the internet and websites
inparticular that provide information, just as
posters, publications and leaflets once did
exclusively. A person’s behaviour may be a result
of interaction with a website and it is considered
part of the record of the activity.
For this reason, websites form part of the record
keeping system and must be preserved. It is also
important to know what material was present
on the website as this material is considered to
have been published. Therefore, the frequency
of capture must be adequate or there must be
some other method to recreate what the website
or intranet visitor viewed. Most NHS organisations’
web sites in Wales are monitored and captured by
the National Library of Wales and are stored in the
UK Web Archive.
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202277
Appendix IV:
Records t contrct chnge
Characteristic of new service
provider
Fair processing required What to transfer Sensitive records
NHS Wales Provider from
same premises and involving
the same sta. This may
be a merger or regional
reconfiguration.
Light: notice on appointment
letter explaining that there is a
new provider. Localpublicity
campaigns such as signage or
posters located on premises.
Entire record or summary of
entire caseload.
N/A
Non-NHS Wales Provider from
same premises and involving
the same sta. Thismay
be a merger or regional
reconfiguration.
Light: notice on appointment
letter explaining that
there is a new provider.
Localpublicity campaign
involving signage and poster
and local communications
oradvertising.
Copy or summary of entire
record of current caseload.
Former provider retains the
original record.
N/A
NHS Wales Provider from
dierent premises but with
thesame sta.
Light: notice on appointment
letter explaining that
there isa new provider.
Localpublicity campaign
involving signage and poster
and local communications
oradvertising.
Copy or summary of entire
record ofcurrent caseload.
Formerprovider retains the
originalrecord.
N/A
RECORDS MANAGEMENT CODE OF PRACTICE FOR HEALTH AND SOCIAL CARE 202278
Characteristic of new service
provider
Fair processing required What to transfer Sensitive records
NHS Wales Provider from
dierent premises and
dierentsta.
Moderate: a letter informing
patients of the transfer with an
opportunity to object or talk to
someone about the transfer.
Copy or summary of entire
record of current caseload.
Allrecords must be
transferred by the former
provider to the new provider.
Individual communications
may not be possible so
obtaining consent, from
the holder of the current
caseload, mayneed to be
sought by the old provider
before transfer. It may not
be possible to transfer the
record without consent, to
satisfy confidentiality, so in
some cases no records will
betransferred.
Non-NHS Wales provider from
dierent premises but with
same sta.
Moderate: a letter informing
patients of the transfer with an
opportunity to object or talk to
someone about the transfer.
Copy or summary of entire
record of current caseload.
Non-NHS Wales from dierent
premises and with dierent
sta.
High: a letter informing
patients of the transfer with an
opportunity to object or talk to
someone about thetransfer.
Copy or summary of entire
record of current caseload.
