
6
OTHER DRUG POLICY ISSUES
2020
© United Nations, June 2020. All rights reserved worldwide.
ISBN: 978-92-1-148345-1
eISBN: 978-92-1-005047-0
United Nations publication, Sales No. E.20.XI.6
This publication may be reproduced in whole or in part and in any form
for educational or non-profit purposes without special permission from
the copyright holder, provided acknowledgement of the source is made.
The United Nations Office on Drugs and Crime (UNODC) would appreciate
receiving a copy of any publication that uses this publication as a source.
Suggested citation:
World Drug Report 2020 (United Nations publication, Sales No. E.20.XI.6).
No use of this publication may be made for resale or any other commercial purpose
whatsoever without prior permission in writing from UNODC.
Applications for such permission, with a statement of purpose and intent of the reproduction,
should be addressed to the Research and Trend Analysis Branch of UNODC.
DISCLAIMER
The content of this publication does not necessarily reflect the views or
policies of UNODC or contributory organizations, nor does it imply any endorsement.
Comments on the report are welcome and can be sent to:
Division for Policy Analysis and Public Affairs
United Nations Office on Drugs and Crime
PO Box 500
1400 Vienna
Austria
Tel: (+43) 1 26060 0
Fax: (+43) 1 26060 5827
E-mail: [email protected]
Website: www.unodc.org/wdr2020
1
PREFACE
This is a time for science and solidarity, as United
Nations Secretary-General António Guterres has said,
highlighting the importance of trust in science and
of working together to respond to the global COVID-
19 pandemic.
The same holds true for our responses to the world
drug problem. To be effective, balanced solutions to
drug demand and supply must be rooted in evidence
and shared responsibility. This is more important
than ever, as illicit drug challenges become increas-
ingly complex, and the COVID-19 crisis and
economic downturn threaten to worsen their impacts,
on the poor, marginalized and vulnerable most of all.
Some 35.6 million people suffer from drug use dis-
orders globally. While more people use drugs in
developed countries than in developing countries,
and wealthier segments of society have a higher preva-
lence of drug use, people who are socially and
economically disadvantaged are more likely to develop
drug use disorders.
Only one out of eight people who need drug-related
treatment receive it. While one out of three drug users
is a woman, only one out of five people in treatment
is a woman. People in prison settings, minorities,
immigrants and displaced people also face barriers to
treatment due to discrimination and stigma. Of the
11 million people who inject drugs, half of them are
living with hepatitis C, and 1.4 million with HIV.
Around 269 million people used drugs in 2018, up
30 per cent from 2009, with adolescents and young
adults accounting for the largest share of users. More
people are using drugs, and there are more drugs, and
more types of drugs, than ever.
Seizures of amphetamines quadrupled between 2009
and 2018. Even as precursor control improves glob-
ally, traffickers and manufacturers are using designer
chemicals, devised to circumvent international con-
trols, to synthesize amphetamine, methamphetamine
and ecstasy. Production of heroin and cocaine remain
among the highest levels recorded in modern times.
The growth in global drug supply and demand poses
challenges to law enforcement, compounds health
risks and complicates efforts to prevent and treat drug
use disorders.
At the same time, more than 80% of the world’s
population, mostly living in low- and middle-income
countries, are deprived of access to controlled drugs
for pain relief and other essential medical uses.
Governments have repeatedly pledged to work
together to address the many challenges posed by the
world drug problem, as part of commitments to
achieve the Sustainable Development Goals, and most
recently in the 2019 Ministerial Declaration adopted
by the Commission on Narcotic Drugs (CND). But
data indicates that development assistance to address
drug control has actually fallen over time.
Balanced, comprehensive and effective responses to
drugs depend on governments to live up to their
promises, and provide support to leave no one behind.
Health-centred, rights-based and gender-responsive
approaches to drug use and related diseases deliver
better public health outcomes. We need to do more
to share this learning and support implementation,
most of all in developing countries, including by
strengthening cooperation with civil society and
youth organizations.
The international community has an agreed legal
framework and the commitments outlined in the
2019 CND Ministerial Declaration. The United
Nations Office on Drugs and Crime (UNODC) pro-
vides integrated support to build national capacities
and strengthen international cooperation to turn
pledges into effective action on the ground.
The theme for this year’s International Day against
Drug Abuse and Illicit Trafficking, “Better Knowledge
for Better Care”, highlights the importance of scien-
tific evidence to strengthen responses to the world
drug problem and support the people who need us.
It also speaks to the ultimate goal of drug control,
namely the health and welfare of humankind.
Through learning and understanding we find com-
passion and seek solutions in solidarity.
It is in this spirit that I present the UNODC World
Drug Report 2020, and I urge governments and all
stakeholders to make the best use of this resource.
Ghada Waly
Executive Director
United Nations Office on Drugs and Crime
Acknowledgements
The World Drug Report 2020 was prepared by the Research and Trend Analysis Branch, Division for
Policy Analysis and Public Affairs, United Nations Office on Drugs and Crime (UNODC), under the
supervision of Jean-Luc Lemahieu, Director of the Division, and Angela Me, Chief of the Research and
Trend Analysis Branch, and the coordination of Chloé Carpentier, Chief of the Drug Research Section.
Content overview
Chloé Carpentier
Angela Me
Analysis and drafting
Andrada-Maria Filip
Jaqueline Garcia-Yi
Barbara Hastie (Indiana University)
Kamran Niaz
Thomas Pietschmann
Editing
Jonathan Gibbons
Graphic design and production
Anja Korenblik
Suzanne Kunnen
Kristina Kuttnig
Federica Martinelli
Administrative support
Iulia Lazar
Review and comments
The World Drug Report 2020 benefited from the expertise of and invaluable contributions from
UNODC colleagues in all divisions.
The Research and Trend Analysis Branch acknowledges the invaluable contributions and advice
provided by the World Drug Report Scientific Advisory Committee:
Jonathan Caulkins
Paul Griffiths
Marya Hynes
Vicknasingam B. Kasinather
Charles Parry
Afarin Rahimi-Movaghar
Peter Reuter
Alison Ritter
Francisco Thoumi
The analysis on access to controlled medicines in Booklet 6 is based on original data graciously shared
by INCB and benefitted from the contribution of the Walther Center in Global Palliative Care of the
University of Indiana.

3
CONTENTS
BOOKLET 1
EXECUTIVE SUMMARY, IMPACT OF COVID-19, POLICY IMPLICATIONS
BOOKLET 2
DRUG USE AND HEALTH CONSEQUENCES
BOOKLET 3
DRUG SUPPLY
BOOKLET 4
CROSS-CUTTING ISSUES: EVOLVING TRENDS AND NEW CHALLENGES
BOOKLET 5
SOCIOECONOMIC CHARACTERISTICS AND DRUG USE DISORDERS
BOOKLET 6
OTHER DRUG POLICY ISSUES
PREFACE ..................................................................................................................... 1
EXPLANATORY NOTES .............................................................................................. 5
SCOPE OF THE BOOKLET........................................................................................... 7
ACCESS TO CONTROLLED MEDICINES FOR PAIN MANAGEMENT .......................... 9
Global amounts of pharmaceutical opioids available for consumption ...................................... 9
Barriers to access to and availability of controlled medicines for pain management
and palliative care .......................................................................................................................... 16
INTERNATIONAL COOPERATION ............................................................................ 22
Extent of implementation of international cooperation is mainly quantified
in terms of specific supply-side measures taken by law enforcement ....................................... 22
Development assistance dedicated to drug control has declined .............................................. 30
Has international cooperation led to global quantities of drugs seized growing
faster than global drug production? ............................................................................................ 35
ALTERNATIVE DEVELOPMENT ................................................................................ 37
Factors influencing resilience to illicit crop cultivation ............................................................... 38
Overview of alternative development projects in the period 2013–2017 ................................. 40
DRUGS AND VIOLENCE ........................................................................................... 48
The tripartite framework on drugs and violence ........................................................................ 48
Economic compulsive and psychopharmacological links between
psychoactive substances, violence and criminal activity .............................................................. 49
The systemic link: violence in the context of drug trafficking ................................................... 53
DRUGS AND THE CRIMINAL JUSTICE SYSTEM ....................................................... 56
Cannabis is the drug that brings most people into contact with the
criminal justice system at the global level ................................................................................... 56
Women who are incarcerated for drug-related offences suffer long-lasting consequences ... 57
GLOSSARY ................................................................................................................ 59
REGIONAL GROUPINGS ........................................................................................... 61

5
EXPLANATORY NOTES
The designations employed and the presentation of
the material in the World Drug Report do not imply
the expression of any opinion whatsoever on the
part of the Secretariat of the United Nations con-
cerning the legal status of any country, territory, city
or area, or of its authorities, or concerning the delim-
itation of its frontiers or boundaries.
Countries and areas are referred to by the names
that were in official use at the time the relevant data
were collected.
Since there is some scientific and legal ambiguity
about the distinctions between “drug use”, “drug
misuse” and “drug abuse”, the neutral term “drug
use” is used in the World Drug Report. The term
“misuse” is used only to denote the non-medical use
of prescription drugs.
All uses of the word “drug” and the term “drug use”
in the World Drug Report refer to substances con-
trolled under the international drug control
conventions, and their non-medical use.
All analysis contained in the World Drug Report is
based on the official data submitted by Member
States to the UNODC through the annual report
questionnaire unless indicated otherwise.
The data on population used in the World Drug
Report are taken from: World Population Prospects:
The 2019 Revision (United Nations, Department of
Economic and Social Affairs, Population Division).
References to dollars ($) are to United States dollars,
unless otherwise stated.
References to tons are to metric tons, unless other-
wise stated.
The following abbreviations have been used in the
present booklet:
AIDS acquired immunodeficiency
syndrome
ATS amphetamine-type stimulants
EMCDDA European Monitoring Centre for
Drugs and Drug Addiction
FARC Revolutionary Armed Forces of
Colombia
ha hectares
HIV human immunodeficiency virus
INCB International Narcotics Control
Board
INTERPOL International Criminal Police
Organization
OECD Organisation for Economic
Co-operation and Development
REDD+ UN Programme on Reducing
Emissions from Deforestation and
Forest Degradation
S-DDD defined daily doses for statistical
purposes
UNDP United Nations Development
Programme
UNODC United Nations Office on Drugs
and Crime
UNESCO United Nations Educational,
Scientific and Cultural Organization
WHO World Health Organization

7
SCOPE OF THE BOOKLET
This, the sixth booklet of the World Drug Report
2020, addresses a number of drug policy issues that
all form part of the international debate on the drug
problem and how to address it. Although compre-
hensive data and analysis may not be available for
some of these issues, the following chapters represent
a first attempt to consolidate available evidence
aimed at supporting the international community
in implementing several operational recommenda-
tions, including those contained in the outcome
document of the special session of the General
Assembly, held in 2016.
The booklet starts by considering the issue of ensur-
ing the availability of and access to controlled
substances exclusively for medical and scientific pur-
poses while preventing their diversion. It thus
reviews the latest data on and trends in the availabil-
ity of controlled medicines, specifically opioids, for
medical consumption at the global level and across
regions. An overview is also provided of the latest
survey findings on barriers to access to controlled
medicines for medical purposes in Member States.
Continuing with the strengthening of international
cooperation based on the principle of common and
shared responsibility, the booklet presents selected
data on international cooperation. The focus of this
chapter is rather limited considering the potentially
wide scope of the topic. It starts with an analysis of
trends with respect to a selected number of inter-
ventions in the area of drug supply reduction, on
which Member States are explicitly asked to report
annually to UNODC through the annual report
questionnaire. The chapter subsequently reviews the
financial means made available by donor countries
for international cooperation on drug issues, before
concluding with an analysis of interceptions trends,
a possible indicator of the success of international
cooperation.
The booklet then provides evidence to support the
implementation of operational recommendations
on alternative development and other development
and socioeconomic issues. This chapter presents the
findings of ongoing research aimed at assessing the
impact of alternative development projects in a
number of countries across different regions affected
by the illicit cultivation of opium poppy or coca
bush. It also provides an overview of the socioeco-
nomic drivers of illicit crop cultivation while
highlighting the specific vulnerabilities of the
affected communities and providing a first-ever esti-
mate of their potential size.
The booklet continues with a discussion of the nexus
between drugs and violence, starting from a con-
ceptual standpoint, and presenting research findings
that illustrate the different mechanisms at play. The
booklet then concludes with a short focus on drugs
and the criminal justice system, including estimates
of people arrested, convicted and held in prison for
drug offences, and a brief overview of the long-
lasting consequences of imprisonment for women
incarcerated for drug law offences.

9
Access to controlled medicines for pain management
6
period 1998–2010 was of oxycodone (which
experienced a tenfold growth over that period),
hydromorphone (fivefold growth), hydrocodone
(threefold growth) and oxymorphone (46,000-fold
growth). Methadone and buprenorphine, the
opioids used in medically assisted treatment of
opioid use disorders, also saw marked increases in
the amounts available for medical consumption at
the global level. The amount of fentanyl available
for medical consumption rose ninefold over the
period 1998–2010.
5
Moreover, since 2000, only
about 10 per cent of globally available morphine
was reported to have been used for palliative care,
5 Narcotic Drugs 2019: Estimated World Requirements for 2020
– Statistics for 2018 (E/INCB/2019/2), and previous years.
ACCESS TO CONTROLLED
MEDICINES FOR PAIN
MANAGEMENT
For nearly six decades, high-level declarations have
been made that affirm the international community’s
collective goal of a balanced, integrated, compre-
hensive, multidisciplinary and scientific
evidence-based approach to controlled medicines,
especially with respect to access and availability for
medical and scientific purposes. Despite recent
growing global advocacy, high-level statements of
intent and movements within international bodies
and individual countries to address access to and
availability of controlled medicines for pain man-
agement, progress has been extremely slow and
significant challenges and barriers remain in improv-
ing the accessibility and availability of controlled
medicines.
1, 2, 3, 4
Global amounts of pharma-
ceutical opioids available for
consumption
Access to and availability of controlled medicines
for pain relief, i.e., opioids, are unequally distributed
across the geographical regions and have had diverg-
ing trends in different regions. The amount of
opioids (expressed in daily doses) available for con-
sumption for medical purposes more than doubled
globally over the period 1998–2010, followed by a
period of stabilization and a decline over the period
2014–2018.
Most of the increase in the amount of pharmaceutical
opioids available for medical consumption over the
1 James F. Cleary and Martha A. Maurer, “Pain and policy
studies group: two decades of working to address regula-
tory barriers to improve opioid availability and accessibility
around the world”, Journal of Pain Symptoms Management,
vol. 55, No. 2 (February 2018), pp. S121–S134.
2 Lilian De Lima and Lukas Radbruch, “Palliative care in
the Global Health Agenda”, Journal of Pain and Palliative
Care Pharmacotherapy, vol. 28, No. 4 (October 2014), pp.
384–389.
3 Liiz Gwyther, Frank Brennan and Richard Harding,
“Advancing palliative care as a human right”, Journal of Pain
Symptom Management, vol. 38, No. 5 (September 2009),
pp. 767–774.
4 Human Rights Watch, “Please Do Not Make Us Suffer Any-
more…”: Access to Pain Treatment as a Human Right (March
2009).
Fig. 1
Global amounts available for medical consump-
tion of pharmaceutical opioids under international
control, 1998–2018
Source: Narcotic Drugs 2019: Estimated World Requirements for 2020 –
Statistics for 2018 (E/INCB/2019/2).
Note: S-DDD refers to “defined daily doses for statistical purposes” as defined by
INCB. S-DDDs are “technical units of measurement” for the purposes of statistical
analysis and are not recommended daily prescription doses; actual doses may differ
based on treatments required and medical practices. The statistics exclude prepara-
tions of opioids listed in Schedule III of the 1961 Convention. Details of S-DDDs
used for these calculations are provided in the methodological annex of the present
report.
a
Substances used as analgesics, i.e., excluding substances used in opioid substitu-
tion treatment.
b
Substances used in opioid substitution treatment and as analgesics.
0
2,000
4,000
6,000
8,000
10,000
12,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
Millions of S-DDD
Methadoneb
Synthetic opioids (analgesics)a
Buprenorphineb
Opiates (analgesics)a
All opiates
All opioids
Methadone
b
Synthec opioids (analgesics)
a
Buprenorphine
b
Opiates (analgesics)
a
All opiates
All opioids

10
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
Fig. 2
Global amounts available for medical consumption of selected opioids
(including preparations), 1998–2018
Source: Narcotic Drugs 2018: Estimated World Requirements for 2019 – Statistics for 2017 (E/INCB/2018/2), and previous years.
Note: All these substances are controlled under the 1961 Convention.
Morphine Codeine
Oxycodone Hydrocodone
Hydromorphone Oxymorphone
Fentanyl Pethidine
0
5,000
10,000
15,000
20,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
0
500
1,000
1,500
2,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
0
500
1,000
1,500
2,000
2,500
3,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
0
1,000
2,000
3,000
4,000
5,000
6,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
0
10,000
20,000
30,000
40,000
50,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
0
20,000
40,000
60,000
80,000
100,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
0
20,000
40,000
60,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
Morphine, including preparations
Morphine
0
100,000
200,000
300,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
Codeine, including preparations
Codeine
Kilograms Kilograms Kilograms
Kilograms
Kilograms
Kilograms
Kilograms Kilograms
11
Access to controlled medicines for pain management
6
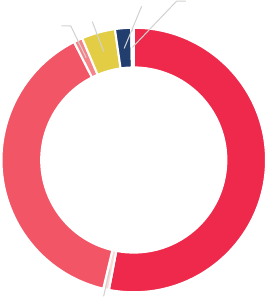
Fig. 3
Distribution of amounts available for medical
consumption of codeine, fentanyl, morphine,
pethidine and other opioids, expressed in stand-
ard defined daily doses (S-DDD), per subregion,
2018
Source: UNODC calculations based on Narcotic Drugs 2019: Estimated
World Requirements for 2020 – Statistics for 2018 (E/INCB/2019/2).
Note: S-DDD refers to “defined daily doses for statistical purposes” as defined
by INCB. S-DDDs are “technical units of measurement” for the purposes of sta-
tistical analysis and are not recommended daily prescription doses; actual doses
may differ based on treatments required and medical practices. Details of
S-DDDs used for these calculations are provided in the methodological annex
of the present report.
There is a gaping chasm between countries in the
availability of opioids for medical purposes. On the
basis of data on the amount of opioids available for
medical purposes, there is a clear disparity between
high-income countries versus low- and middle-
income countries
12
for all opioids combined (i.e.,
codeine, fentanyl, hydromorphone, morphine, oxy-
codone, pethidine and methadone).
Data for 2018 show that more than 90 per cent of
all pharmaceutical opioids that are available for med-
ical consumption are in high-income countries: 50
per cent in North America, around 40 per cent in
Europe, mostly in Western and Central Europe, and
a further 2 per cent in Oceania, mostly Australia
and New Zealand. Those high-income countries
11 See, for example, World Drug Report 2018 (United Nations
publication, Sales No. E.18.XI.9).
12 Based on the country classification 2014 of the World Bank
Country and Lending Groups.
while over 88 per cent was converted into codeine,
the majority of which (89 per cent) was used to
manufacture cough medicines.
6
Since 2014, the decline in the amount of opioids
available for medical consumption has been par-
ticularly pronounced for oxycodone, hydrocodone
and hydromorphone, following stricter rules aimed
at reducing diversion in North America. Prior to
that, these substances were heavily diverted to mar-
kets for non-medical use, particularly in North
America. Nonetheless, in 2018 that subregion con-
tinued to account for a major share of the global
amounts available for medical consumption of
hydromorphone (69 per cent), oxycodone (69 per
cent) and hydrocodone (99 per cent).
7
The amounts available for medical consumption of
some of the other synthetic opioids used in pain
management have been declining over the past two
decades. Pethidine is one example, with a 70 per
cent decline over the period 1998–2018, while
amounts available for medical consumption of dex-
tropropoxyphene, which was very popular in the
1990s, have decreased by more than 99 per cent
over the past two decades as the substance was
banned in a number of countries owing to concerns
over serious side effects.
8
The amount of fentanyl
available for medical consumption increased until
2010 but remained largely stable thereafter.
9
By contrast, the amounts of buprenorphine and
methadone available for medical consumption and
used in the medically assisted treatment of opioid
use disorders, have increased since 2014, especially
of buprenorphine, which rose by more than 50 per
cent over the period 2014–2018.
10
However, as with
other pharmaceutical opioids, there are large differ-
ences from one country to another in the
consumption patterns of buprenorphine and metha-
done for medical purposes, as seen in the coverage
of opioid-agonist treatment for people with opioid
use disorders.
11
6 Progress in Ensuring Adequate Access to Internationally
Controlled Substances for Medical and Scientific Purposes
(E/INCB/2018/Supp.1).
7 Ibid.
8 E/INCB/2019/2.
9 Narcotic Drugs 2018: Estimated World Requirements for 2019
– Statistics for 2017 (E/INCB/2018/2), and previous years.
10 Ibid.
North
America
53%
South America, Central
America, Caribbean
1%
Western
and
Central
Europe
39%
Eastern and
South-Eastern
Europe
1%
Asia
4%
Oceania
2%
Africa
0.3%

12
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
comprise around 12 per cent of the global popula-
tion. Therefore, low- and middle-income countries,
which are home to some 88 per cent of the global
population, are estimated to consume less than 10
per cent of the global amount of opioids available
for medical consumption.
Even within each region or subregion, there is a
significant disparity in the consumption of opioids
for medical purposes. Over the period 2014–2018,
average consumption of opioids in countries in
North America ranged from some 100 defined daily
doses for statistical purposes (S-DDD) per million
inhabitants in Mexico to 32,700 S-DDD per mil-
lion inhabitants in the United States of America.
Similarly, in Western and Central Europe, estimates
ranged from close to 500 S-DDD per million inhab-
itants in Malta to 25,800 S-DDD per million
inhabitants in Germany. In Oceania, estimates
ranged from, on average, 15 S-DDD per million
inhabitants in Vanuatu to close to 11,600 S-DDD
per million inhabitants in Australia, and in Asia,
from 0.1 S-DDD per million inhabitants in Yemen
to close to 11,300 S-DDD per million inhabitants
in Israel.
Data show that there is a generally positive correla-
tion between gross national income and the
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
S-DDD per million inhabitants
North America
Western and
Central Europe
Oceania
East and South-eastern
Europe
South America, Central
America and the Caribbean
Asia
Africa
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
0 20,000 40,000 60,000 80,000 100,000
S-DDD per million inhabitants
Gross national income (GNI) per capita in current dollars
Fig. 5
Amounts available for medical consumption of
codeine, fentanyl, morphine, pethidine and other
opioids in individual countries, and per capita
income, average 2014–2018
Source: UNODC calculations based on Narcotic Drugs 2019: Estimated
World Requirements for 2020 – Statistics for 2018 (E/INCB/2019/2).
Note: S-DDD refers to “defined daily doses for statistical purposes” as defined
by INCB. S-DDDs are “technical units of measurement” for the purposes of sta-
tistical analysis and are not recommended daily prescription doses; actual doses
may differ based on treatments required and medical practices. Details of
S-DDDs used for these calculations are provided in the methodological annex of
the present report.
Fig. 4
Distribution of amounts available for medical consumption of codeine, fentanyl, morphine,
pethidine and other opioids, per country, 2018
Source: UNODC calculations based on Narcotic Drugs 2019: Estimated World Requirements for 2020 – Statistics for 2018
(E/INCB/2019/2).
Note: S-DDD refers to “defined daily doses for statistical purposes” as defined by INCB. S-DDDs are “technical units of measurement” for
the purposes of statistical analysis and are not recommended daily prescription doses; actual doses may differ based on treatments
required and medical practices. Details of S-DDDs used for these calculations are provided in the methodological annex of the present
report.
13
Access to controlled medicines for pain management
6
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
North America
Western and Central Europe
Australia and New Zealand
Global average
South-Eastern Europe
Near and Middle East/ South-West Asia
South America
Eastern Europe
Caribbean
East and South-East Asia
Central America
Melanesia, Polynesia and Micronesia
Africa
South-Asia
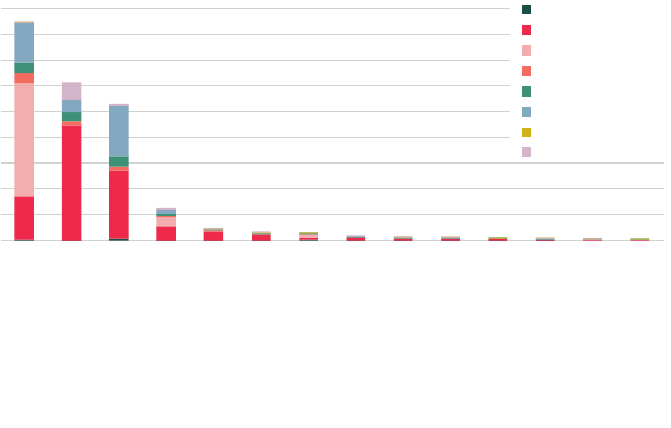
S-DDD per million inhabitants
Codeine
Fentanyl
Hydrocodone
Hydromorphone
Morphine
Oxycodone
Pethidine
Other
North America
Western and
Central Europe
Australia and
New Zealand
Global average
South-Eastern
Europe
Near and Middle East/
South-West Asia
South America
Eastern Europe
Caribbean
East and
South-East Asia
Central America
Melanesia, Polynesia
and Micronesia
Africa
South-Asia
the availability of codeine for medical consumption
appears to be quite limited, although this may be a
statistical artefact as most codeine is sold in the form
of preparations, the sale of which – falling under
Schedule III of the 1961 Single Convention – is
internationally less strictly controlled and thus less
well documented than the sale of other pharmaceu-
tical opioids.
There have been concerted international and coun-
try-level efforts to address the inequity in the
consumption of pharmaceutical opioids,
13
particu
-
larly in the case of morphine, which has been on
the WHO Model List of Essential Medicines for
management of pain due to cancer, HIV/AIDS and
other serious illnesses, and due to traumatic injuries,
burns and surgery, for nearly two decades.
14, 15
Despite this, morphine has not been accessible in
13 Cleary and Maurer, “Pain and policy studies group”.
14 De Lima and Radbruch, “Palliative care in the Global
Health Agenda”.
15 WHO, World Health Organization Model List of Essential
Medicines: 21th List (Geneva, 2019).
availability of pharmaceutical opioids for medical
purposes (R=0.67 over the period 2014–2018),
although a number of Asian countries and territories
with high gross national income per capita (such as
Macao, China, Hong Kong, China, Qatar, Singa-
pore, Japan and Kuwait) have very low levels of
opioid availability for medical purposes. This sug-
gests that the level of national income is not the
only factor that explains unequal availability across
countries. A number of barriers to access to opioids
for pain management are related to legislation, cul-
ture, health systems and prescribing practices.
Data also show discrepancies in the kind of phar
-
maceutical opioids available on the medical market.
While data for North America show that hydroco-
done is the most widely available pharmaceutical
opioid (in terms of daily doses per inhabitant), fen-
tanyl is the most widely available opioid in Western
and Central Europe and in Australia and New Zea-
land. The availability for medical consumption of
oxycodone is also relatively high in Australia and
New Zealand and in North America. By contrast,
Fig. 6
Amounts available for medical consumption of codeine, fentanyl, morphine, pethidine and
other opioids, by region and subregion,
a
2018
Source: UNODC calculations based on Narcotic Drugs 2019: Estimated World Requirements for 2020 – Statistics for 2018
(E/INCB/2019/2).
Note: S-DDD refers to “defined daily doses for statistical purposes” as defined by INCB. S-DDDs are “technical units of measurement” for
the purposes of statistical analysis and are not recommended daily prescription doses; actual doses may differ based on treatments
required and medical practices. Details of S-DDDs used for these calculations are provided in the methodological annex of the present
report
a
The regions and subregions are those designated by UNODC in the World Drug Report; they may partly differ from those used by INCB
in its publications.

14
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
the amounts of morphine available for medical con-
sumption in low- and middle-income countries has
increased slightly since 2014 (from 9.5 to 13 per
cent in 2018) the amount of morphine available per
person per country is still infinitesimally small to
non-existent in many developing countries, particu-
larly in South Asia and in Africa.
18, 19
Even though
countries may have morphine available for medical
use, many people still have limited access to it.
20, 21
WHO estimates that globally, each year 5.5 million
18 E/INCB/2018/Supp.1.
19 E/INCB/2019/2.
20 See section below on barriers to access to and availability of
controlled medicines for pain management and palliative
care.
21 E/INCB/2019/2.
adequate amounts, in the appropriate dosage forms,
with assured quality and adequate information and
at a price that an individual and the community can
afford.
16, 17
In 2018, 87 per cent of the global amount of mor-
phine available for medical consumption was
estimated to have been consumed in high-income
countries, which are home to 12 per cent of the
global population. While the relative importance of
16 WHO, Integrating Palliative Care and Symptom Relief into
Primary Health Care: A WHO Guide for Planners, Imple-
menters and Managers (Geneva, 2018).
17 Felicia Marie Knaul and others, “Alleviating the access abyss
in palliative care and pain relief: an imperative of universal
health coverage – the Lancet Commission report”, Lancet,
vol. 391, No. 10128 (April 2018).
Fig. 7
Trends in availability of opioid analgesics for medical consumption, by region/subregion,
a
1998–2018
Source: UNODC calculations based on Narcotic Drugs 2019: Estimated World Requirements for 2020 – Statistics for 2018 (E/
INCB/2019/2) and previous years.
Note: S-DDD refers to “defined daily doses for statistical purposes” as defined by INCB. S-DDDs are “technical units of measurement” for
the purposes of statistical analysis and are not recommended daily prescription doses; actual doses may differ based on treatments
required and medical practices. Details of S-DDDs used for these calculations are provided in the methodological annex of the present
report.
a
Subregions and regions according to the classification used by UNODC in the World Drug Report; subregions and regions as defined
partly differ from those used by INCB in its publications; extrapolation techniques have been used in case of missing data.
b
Includes subregions above the global average, i.e., North America, Western and Central Europe, Australia and New Zealand.
c
Includes regions and or subregions below the global average, i.e., Africa, Asia, Eastern Europe, South-Eastern Europe, the Caribbean,
Central America and South America, as well as Melanesia, Micronesia and Polynesia, i.e., all regions and subregions except those of North
America, Western and Central Europe, and Australia and New Zealand.
High-consumption subregions
b
Low-consumption regions/subregions
c
0
200
400
600
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
S-DDD per million inhabitants
Eastern and South-Eastern Europe
South America, Central America and Caribbean
Near and Middle East/South-West Asia
East and South-East Asia
Oceania excluding Australia and New Zealand
Africa
South Asia
Central Asia and Transcaucasia
0
10,000
20,000
30,000
40,000
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
S-DDD per million inhabitants
North America
Western and Central Europe
Australia and New Zealand
Other countries
Global average

15
The role of complementary and alternative medicine in the
management of chronic non-cancer pain
The use of strong opioids, especially morphine, is gener-
ally considered the principal treatment for the manage-
ment of pain in palliative care for cancer patients.
a
The
treatment of chronic non-cancer pain, which is among
the most prevalent health conditions in many countries,
is often considered more difficult to manage, and its
treatment is sometimes more controversial.
b
Chronic
non-cancer pain is defined in scientific literature as pain
lasting for more than three months that stems from
injuries or illnesses other than cancer.
c
It is also consid-
ered that chronic pain results from a combination of
biological, psychological and social factors, and thus
requires a multifactorial approach to pain assessment,
patient monitoring and evaluation and long-term man-
agement. Some of the common conditions that cause
chronic pain include neuropathic pain, fibromyalgia
that may be caused by damage to the peripheral or cen-
tral nervous system, low back pain and osteoarthritis.
While opioids are used extensively in the management
of non-cancer chronic pain in some countries and set-
tings, in others, other drugs, as well as complementary
and alternative medicines, are used effectively in the
management of chronic pain whether related to cancer
or not.
d, e
Other than opioids, non-steroidal anti-inflammatory
drugs are used in patients with osteoarthritis and rheu-
matoid arthritis and low back pain. The efficacy of anti-
depressant drugs has been reported for the management
of neuropathic pain, fibromyalgia, low back pain and
headaches. Anti-convulsant drugs such as gabapentin,
pregabalin and carbamazepine have proved effective in
the treatment of chronic non-cancer pain.
f
As part of complementary and alternative medicine,
spinal manipulation is the most commonly used therapy
for low back pain.
g
Massage is another modality com-
monly used as a supplemental treatment for patients
with chronic non-cancer pain. Similarly, evidence sup-
ports the effectiveness of acupuncture for the treatment
of chronic low back pain, while results on the effective-
ness of acupuncture in the reduction of pain associated
with fibromyalgia and neck pain are promising.
h
Psychological interventions such as cognitive behav-
ioural therapy, relaxation training and hypnosis are the
most commonly used techniques in the management of
chronic pain.
i
The aim of such interventions is to help
the patient cope with the symptoms of pain, learn skills
for adaptation and self-management, and reduce disa-
bility associated with symptoms, rather than eliminate
physical causes of pain per se.
j
a
WHO, Ensuring Balance in National Policies on Controlled Sub-
stances: Guidance on Availability and Accessibility of Controlled
Medicines (Geneva, 2011).
b
Nora D. Volkow and A. Thomas McLellan, “Opioid abuse in
chronic pain: misconceptions and mitigation strategies”, New
England Journal of Medicine, vol. 374, No. 13 (March 2016), pp.
1253–1263.
c
Dennis C. Turk, Hilary D. Wilson and Alex Cahana, “Treatment
of chronic non-cancer pain”, Lancet, vol. 377, No. 9784 (June
2011), pp. 2226–2235.
d
Ibid.
e
Priyanka Singh and Aditi Chaturvedi, “Complementary and
alternative medicine in cancer pain management: a systematic
review”, Indian Journal of Palliative Care, vol. 21, No. 1 (2015),
pp. 105–115 (2015).
f
Turk, Wilson and Cahana, “Treatment of chronic non-cancer
pain”.
g
Ibid.
h
Ibid.
i
Singh and Chaturvedi, “Complementary and alternative medicine
in cancer pain management”.
j
Turk, Wilson and Cahana, “Treatment of chronic non-cancer
pain”.
Access to controlled medicines for pain management
6
available for medical consumption are reported in
North America, while overall increases are reported
in several other subregions, most notably South
America and the Near and Middle East/South-West
Asia, where availability has been low. This suggests
an overall increase in the availability of opioids in
developing countries, although that availability was
starting from, and remains at, a low level. Daily per
capita availability of pharmaceutical opioids more
terminal cancer patients and 1 million end-stage
HIV/AIDS patients do not have adequate treatment
for moderate to severe pain.
22
In recent years the huge disparity between countries
in the accessibility of opioids for medical purposes
has been reduced slightly: declines in opioids
22 WHO, Integrating Palliative Care and Symptom Relief into
Primary Health Care.
16
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
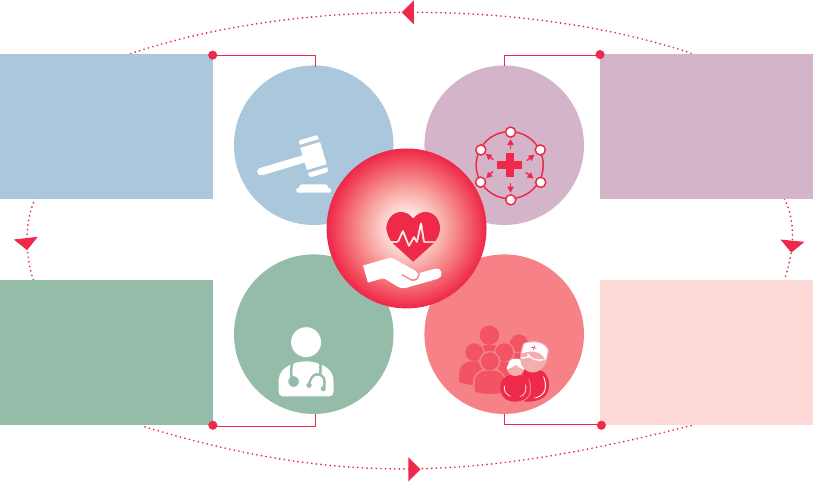
There are several challenges and barriers to access
to controlled medicines for pain management, all
of which are complex, multitiered and interrelated.
These include, but are not limited to, trade systems,
education, justice, foreign affairs, workforce and
development, but perhaps the most recognized and
salient among them are legislation and regulatory
systems, national supply management systems and
health systems. Each of these directly and indirectly
influences the barriers to both access to and avail-
ability of controlled medicines for pain management
and palliative care.
26
These challenges and barriers,
including the progress that has been made globally
to address them, are discussed below.
Legislation and regulatory systems
In 2018, INCB conducted a survey
27
of competent
national authorities in order to assess the barriers
and evaluate progress made at the national level in
improving access to and availability of controlled
substances for pain management since the previous
surveys in 1995, 2010 and 2014. Of the 130 coun-
tries (representing 78 per cent of the global
population) that responded, 40 per cent indicated
that over the previous five years, legislation and/or
regulatory systems had been reviewed or changed
to affect the availability of controlled medicines.
Some countries reported unspecified “general
changes,” others indicated that changes were made
to the status of controlled substances, while some
introduced electronic measures to facilitate prescrip
-
tions and/or procurement.
Although regulations that have limited the
availability of controlled medicine have been reduced
in many countries since 1995, challenges remain.
In 2018, 26 per cent of the countries that responded
to the survey mentioned the existence of legal
sanctions for unintentional errors in handling opioid
analgesics. The legal threat was reported to be a
major factor in the decisions of some doctors not
to procure, stock or prescribe opioids, thus limiting
their access. Similar challenges affect the number of
pharmacies that are willing to dispense opioids.
28
In 2018, the three major impediments to the
26 E/INCB/2018/Supp.1.
27 Ibid.
28 Ibid.
than doubled in the regions and subregions where
availability was below the global average (i.e., Africa,
Asia, South America, Central America, the Carib-
bean, Eastern and South-Eastern Europe, Melanesia,
Micronesia and Polynesia); taken together, availabil-
ity in these regions and subregions increased from
an average of 70 S-DDD per million inhabitants in
2010 to 180 S-DDD in 2018 (7 per cent of the
global per capita average).
23
By contrast, the availability of pharmaceutical opi-
oids for medical purposes declined by almost 50 per
cent in North America, from 32,550 S-DDD per
day per million inhabitants in 2010 to 16,910
S-DDD in 2018, thus approaching the levels
reported in Western and Central Europe (12,660
S-DDD) and in Australia and New Zealand (10,530
S-DDD) in 2018. Nevertheless, per capita availabil-
ity of pharmaceutical opioids for medical purposes
in North America remains comparatively high
(almost eight times the global average), in particular
when compared with the extremely low levels in
Africa and South Asia, as well as in Central Asia and
Transcaucasia, where there are no signs of
increases.
24
INCB notes that the increase in the use of expensive
synthetic opioids over the past two decades, which
has contributed to overconsumption and an “over-
dose epidemic” in some developed countries, has
not been matched by an increase in the use of afford-
able morphine, especially in low- and middle-income
countries.
25
Barriers to access to and
availability of controlled medi-
cines for pain management
and palliative care
The reasons for inequities in access to and availabil-
ity of opioids for pain management are extraordinarily
complex and include historical vestiges across mul-
tiple systems, i.e., government, health care and
society, as well as modern-day challenges, including
the concerns arising out of the opioid overdose crisis.
23 E/INCB/2019/2.
24 Ibid.
25 E/INCB/2018/Supp. 1.
17
Access to controlled medicines for pain management
6
health-care services and/or where the number of
physicians or doctors is limited.
In 2018, INCB also surveyed civil society organiza-
tions and received responses from 30 organizations
based in 23 countries in Asia, Africa, Europe and
the Americas.
31
More than half of the organizations
that responded to the questionnaire reported
changes to, or reviews of, legislation or regulations
aimed at simplifying and streamlining processes and
removing unduly restrictive regulations in order to
ensure accessibility of controlled substances and
maintain adequate control systems in their respec-
tive countries. Although this is a limited sample of
civil society organizations, it demonstrates a rela-
tively positive perception of some of the actions that
countries have taken to change or streamline the
laws and regulations that limit access to and avail-
ability of controlled medicines.
National supply management systems
Functional, effective and efficient national supply
chain management systems that are guided by the
international drug control conventions are critically
important to achieving the balance between prevent-
ing diversion and ensuring adequate access to and
31 Ibid.
availability of opioids, as reported by the countries
responding to the survey, were lack of training and
awareness of health-care professionals, fear of
addiction, and problems in sourcing opioid
medications.
29
Some evidence of progress in improving access to
and availability of controlled medicines for pain
management is suggested in a small proportion (16
per cent) of countries that reported that legislation
and regulations had been modified to broaden the
range of health-care professionals who are allowed
to prescribe controlled substances. Overall, 123
countries reported that they allow medical special-
ists to prescribe controlled substances for pain
management and palliative care, while 98 countries
also allow general practitioners. Challenges continue
to limit the range of health-care providers who can
prescribe opioid analgesics, as only nine countries
surveyed reported that their legislation allowed
nurses, including nurse practitioners, to prescribe
those drugs.
30
This legislative and regulatory limita-
tions on who can prescribe controlled substances
perpetuates a barrier to access, particularly in low-
and middle-income countries without decentralized
29 Ibid.
30 Ibid.
Patient,
family and
community
Health-care
systems and
providers
Supply
management
system
Legal
and
regulatory system
Opioid access
and palliative care
• Disparities in:
- Production/manufacturing
- Distribution channels
- Affordability
• Inadequate/inefficient in-country
monitoring/tracking systems
• Barriers tracking consumption
• Safeguards, storage, stock-outs
• Policies and programmes
• Capacity building and attitude
of health-care workers:
- Physicians
- Nurses and nurse practitioners
- Pharmacists
- Community health workers
- Spiritual care workers
• National policies
• International/national laws and
regulations
• Collaboration with international
organizations
- Competent authorities
work/train with INCB
- Training in-country enforcers
• Accessibility, availability,
affordability
• Patient, family and community
education
• Cultural biases and stigma
• Availability of community health
workers
• Safeguarding medicines
Systems and influences affecting access to and availability of controlled medicines
Systems and influences affecting access to and availability of controlled medicines

18
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
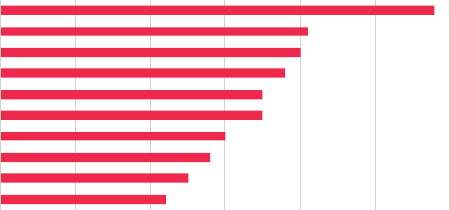
Fig. 9
Health-care providers allowed to prescribe controlled substances, 2018
Source: Progress in Ensuring Adequate Access to Internationally Controlled Substances for Medical and Scientific Purposes
(E/INCB/2018/Supp.1).
Note: The data represent the number of countries who responded to the survey and indicated the kind of health-care providers who can
prescribe controlled substances, including opioids for pain management and palliative care. Multiple responses were possible.
impediments to ensuring the availability of con-
trolled substances. To address this, INCB has
introduced a number of online and electronic sys-
tems to streamline and simplify import and export
processes within countries.
32
One improvement over
the years has been the gradual establishment of elec-
tronic tools for processing import and export
authorizations, with competent national authorities
in 50 countries reporting the use of such tools in
2018. In addition, with a view to facilitating the
production of reliable estimates of the quantities of
controlled substances needed nationally, guidelines
32 These include the National Drug Control System and the
International Import and Export Authorization System
(I2ES).
availability of controlled medicines for pain man-
agement and palliative care. Within national supply
chains and management systems, diverse domains
affect export, import, procurement and monitoring
of access to and availability of controlled medicines,
to name but a few. Within this chain, primary areas
that affect the accessibility of controlled substances
in a country are: (1) processes to produce national
estimates of controlled medicines for pain manage-
ment and palliative care; (2) assessment of the
availability of controlled substances; and (3) devel-
oping benchmarks (compared to thresholds for high
and low use of controlled substances).
Countries report that import and export control
measures or restrictions are among the main
Fig. 8
Reported impediments to the availability of controlled medicines for pain management, 2018
Source: Progress in Ensuring Adequate Access to Internationally Controlled Substances for Medical and Scientific Purposes
(E/INCB/2018/Supp.1).
Note: The percentage represents the proportion of responding countries that mentioned each of the factors as an impediment to the
availability of pain medications. Multiple responses were possible.
0
20 40 60 80 100 120 140
Others
Nurses (including nurse practitioners)
General practitioners (special licence)
Veterinarians
General practitioners
Medical specialists/psychiatrists, oncologists, surgeons, dentists)
Number of countries
Medical specialists/psychiatrists,
oncologists, surgeons, densts)
General praconers
Veterinarians
General praconers (special licence)
Nurses (including nurse praconers)
Others
0 10 20 30 40
Onerous regulations
Fear of prosecution/sanctions
Cultural attitudes
Limited financial resources
Trade control measures
Fear of diversion
Problems in sourcing
Fear of addiction
Lack of training/awareness of professionals
Percentage of countries
Lack of training/awareness of professionals
Fear of addicon
Problems in sourcing
Fear of diversion
Trade control measures
Limited nancial resources
Cultural atudes
Fear of prosecuon/sancons
Onerous regulaons

19
Access to controlled medicines for pain management
6
palliative care was included in the educational cur-
ricula in medical schools. Similarly, 76 countries
reported that continuing education, training and
information on palliative care, including on the
rational use and the importance of reducing the
misuse of prescription drugs, was provided to health-
care professionals. However, 11 countries reported
that education on palliative care was provided for
only a limited number of medical specialities, such
as oncology, and a further 43 countries reported
that palliative care was not included as a discipline
in their medical education programme. While nine
countries reported that they did not have a medical
school, four countries noted that they would build
palliative care into the medical curriculum from the
onset. This demonstrates an awareness, and a con-
certed effort, on the part of the medical profession
of the importance of palliative care training across
the life course of wider medical training.
In addition, 41 countries noted that national com-
petent authorities did not have training programmes
on the rational use of controlled substances and that
this was either due to a lack of resources or because
it was “not a priority” for the Government.
Regarding other fields of specialty with interaction
with patients and which are an important resource
in health-care delivery, especially in low- and middle-
income countries where the availability of doctors
is limited, the nursing profession has made significant
strides in incorporating palliative care and end-of-
life care training, not only in the curriculum for
for estimating the national requirements of con-
trolled substances have also been made available in
recent years.
33
Nevertheless, many countries, for a
myriad of reasons, continue to report to INCB that
they are unable to properly estimate or to monitor
consumption of controlled substances and continue
to inadequately or insufficiently estimate opioid
requirements.
Health systems
Improving the accessibility and availability of con-
trolled substances, including opioids for pain
management and palliative care, also requires
improving health systems to ensure controlled sub-
stances are prescribed and administered in a rational
and efficient manner.
34
Overall, the major steps
taken by countries that responded to the INCB
survey in 2018 included improvements to the health
insurance system and the setting of affordable prices
to improve the accessibility and availability of con-
trolled substances, including opioids for pain
management and palliative care.
Training and capacity-building
The training and capacity-building of health-care
professionals in all domains is key to ensuring access
to and availability of opioids for pain management.
In this regard, 71 countries (or 62 per cent of those
that responded to the INCB survey) reported that
33 INCB and WHO, Guide on Estimating Requirements for
Substances under International Control (Vienna, 2012).
34 E/INCB/2018/Supp. 1.
Fig. 10
Steps taken by countries to improve the accessibility of controlled substances, 2018
Source: Progress in Ensuring Adequate Access to Internationally Controlled Substances for Medical and Scientific Purposes
(E/INCB/2018/Supp.1).
Note: The data represent the number of countries that responded to the survey and indicated the steps taken to improve the accessibility
of controlled substances, including opioids for pain management and palliative care. Multiple responses were possible.
0 10 20 30 40 50
Monitoring and management
Procurement of essential drugs
Awareness-raising and training
Establishment of a list of essential medicines
Amendments to guidelines and legislation
No action
Improvement to the health insurance system and setting of affordable prices
Number of countries
Improvement to the health insurance system
and seng of aordable prices
No acon
Amendments to guidelines and legislaon
Establishment of a list of essenal medicines
Awareness-raising and training
Procurement of essenal drugs
Monitoring and management
20
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
reported by 130 countries.
42
Fear of addiction seems
to be related to a lack of awareness and training, and
to cultural attitudes.
43
These barriers influence all
systems and the people in them, including national
and international policymakers, regulators, health-
care professionals, community advocates, patients
and the public at large.
Moreover, at the global level, concerns over the non-
medical use of pharmaceutical opioids, triggered by
the opioid crisis in North America, North Africa,
and West and Central Africa has created a challenge
for increasing the availability of opioids for pain
management and palliative care due to the concomi-
tance of the two opposing needs. As a result,
low- and middle-income countries, not only in
Africa but also in other regions, some of which have
extremely limited access to opioids, are now facing
diminished access and have to counter increased
fear of addiction – that may result from a lack of
knowledge about substance use disorders and the
science of prevention and treatment – among poli-
cymakers, national authorities, health-care providers
and even among the public.
44, 45, 46, 47
Countries that reported to the 2018 INCB survey
mentioned specific initiatives undertaken by national
competent authorities to enhance the understanding
of, awareness of and education about, and address
cultural resistance to and the stigma associated with,
the use of opioids and other controlled substances:
education for representatives of the pharmaceutical
community, professionals and consumer groups; and
the promotion of ethical attitudes among medical
doctors and pharmaceutical companies, in particular
to reduce the excessive marketing of opioids.
48
42 E/INCB/2018/Supp.1.
43 Availability of Internationally Controlled Drugs: Ensuring
Adequate Access for Medical and Scientific Purposes –
Indispensable, Adequately Available and not Unduly Restricted
(E/INCB/2015/1/Supp.1).
44 Knaul and others, “Alleviating the access abyss in palliative
care and pain relief”.
45 African Palliative Care Association, Guidelines for Ensuring
Patient Access to, and Safe Management of, Controlled Medi-
cines (Kampala, 2013).
46 De Lima and Radbruch, “Palliative care in the Global
Health Agenda”.
47 Pettus and others, “Ensuring and restoring balance on
access to controlled substances for medical and scientific
purposes”.
48 E/INCB/2018/Supp.1.
nurses but also for them to train other health-care
providers within the larger health-care community.
35,
36, 37
For example, many non-governmental
organizations in Africa have initiated programmes
for training community health-care workers in
palliative care, who do not necessarily require
licensure and do not undergo extensive formal
training in medicine, pharmacy or nursing.
38
In
resource-constrained settings, community health-
care workers are considered quite instrumental in
providing care outside urban areas, in villages and
other community settings with limited access to
formal health-care services and facilities.
39
Pharmacy training is gaining attention given the
frontline role of pharmacies in making opioids
accessible for patients. Palliative care training is not
mandatory but many programmes, including by
non-governmental organizations and other advocacy
organizations, are targeting pharmacy professionals.
40
Education and awareness-raising
Lack of awareness and “fear of addiction”, i.e., the
concern that patients who are prescribed strong opi-
oids are likely to develop dependence or iatrogenic
addiction,
41
were reported to be among the top
impediments to access to controlled substances
35 A leading programme is the End-of-Life Nursing Education
Consortium, which is based on a train-the-trainer model
and has been implemented in over 100 countries worldwide.
36 Betty Ferrel, Pam Malloy and Rose Virani, “The end of life
nursing education nursing consortium project”, Annals of
Palliative Medicine, vol. 4, No. 2 (April 2015), pp. 61–69.
37 Henry Ddungu, “Palliative care: what approaches are suit-
able in developing countries?”, British Journal of Haematol-
ogy”, vol. 154, No. 6 (September 2011), pp. 728–735.
38 The African Palliative Care Association is one leading
organization working in this area. See, for instance, Annual
Report: Building Bridges 2017-18 (Kampala, 2019).
39 Katherine Pettus and others, “Ensuring and restoring bal-
ance on access to controlled substances for medical and
scientific purposes: joint statement from palliative care
organizations”, Journal of Pain Palliative Care and Pharmaco-
therapy, vol. 32, No. 2–3 (September 2018), pp. 124–128.
40 African Palliative Care Association, Annual Report: Building
Bridges 2017-18.
41 A structured review of 67 studies found that 3 per cent
of chronic non-cancer patients regularly taking opioids
developed opioid use disorders. See David A. Fishbain and
others, “What percentage of chronic non-malignant pain
patients exposed to chronic opioid analgesic therapy develop
abuse/addiction and/or aberrant drug related behaviours?
A structured evidence-based review”, Pain Medicine, vol. 9,
No. 4 (May 2008), pp. 444-459.
21
Access to controlled medicines for pain management
6
and in most low- and middle-income countries,
where a large number of people are not covered by
either health insurance or a national health-care
system, many people can encounter difficulties in
accessing the pain medications that they need.
50
International cooperation and
coordination
For many years, Governments, academic institutions
and non-governmental organizations have worked
across and within systems nationally and interna-
tionally on the central principle of balance between
access to controlled substances for medical and sci-
entific purposes and prevention of their diversion.
Over the past 20 years, demonstrable progress has
been made in over 30 countries in this regard.
51
Similarly, collaboration between international stake-
holders that aim to improve the legislative
framework, build capacity of health-care profession-
als, and work with patients, families and the public
in order to improve access to and availability of
controlled substances has shown the importance of
working across these major domains. Each of them
could act as an impediment or serve to enable access
to opioids for pain management and palliative care
at the country level.
50 Ibid.
51 Cleary and Maurer, “Pain and policy studies group”.
Affordability
The availability of pain medications is determined
by factors that include their physical availability and
practical accessibility. These in turn depend on the
extent to which pain medications are procured and
the existence of an appropriate and viable health
system. Furthermore, the affordability of those medi-
cations is central to all of the elements, especially in
the context of universal health coverage. Affordabil-
ity is addressed, among other ways, by ensuring
funding for the purchase of opioid medications as
well as developing and improving health insurance
and reimbursement schemes that guarantee access
to pain medication.
49
In 2018, 50 countries reported
to INCB that steps had been taken towards improv-
ing their health insurance systems and setting
affordable prices for essential medicines, including
opioids. However, limited resources can impair even
a well-intended Government from procurement or
preclude it from providing or subsidizing controlled
medicines for pain management. Other issues that
may affect the affordability of pain medications
include licensing, taxation, poor or inefficient dis-
tribution systems, lack of reimbursement and lack
of availability of inexpensive formulations. Even in
the case of Governments that are strongly commit-
ted to addressing challenges and barriers to access,
financial resources may not be available to make
systemic changes. Moreover, because of the high cost
of pain medications, in many high-income countries
49 Ibid.
Fig. 11
Education and awareness-raising initiatives, 2018
Source: Progress in Ensuring Adequate Access to Internationally Controlled Substances for Medical and Scientific Purposes
(E/INCB/2018/Supp.1).
Note: The data represent the number of countries that responded to the survey and indicated the initiatives taken by the competent
national authorities for education and awareness to improve the accessibility of controlled substances, including opioids for pain manage-
ment and palliative care. Multiple responses were possible.
0 10 20 30 40 50 60
Reducing excessive marketing
Overcoming cultural resistance
Reduction of stigma and fear of addiction
Education for the general public
Palliative care education in curricula
Engagement of civil society and non-governmental organizations
Prevention of non-medical use of psychotropic substances
Promotion of ethical attitudes
Media campaigns
Education for pharmaceutical community
Number of countries

22
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
should be kept in mind, even though it is not dis-
cussed further in this chapter.
The purpose of this chapter is to present and exam-
ine the information that countries have regularly
submitted to UNODC on the topic of international
cooperation. Its scope is relatively limited and it does
not pretend to cover the complex nature of factors
that influence the implementation of international
cooperation measures and their outcomes.
Extent of implementation of
international cooperation is
mainly quantified in terms of
specific supply-side measures
taken by law enforcement
Reporting on the implementation of international
cooperation globally is challenging because interna-
tional cooperation can take different forms, which
are difficult to measure. For example, the sharing of
intelligence information, probably the most common
form of cooperation to address drug-related matters,
happens in day-to-day work within and across law
enforcement agencies; and it is hardly recorded in
any systematic way at the national level in most coun-
tries. Records exist of some forms of
intelligence-sharing at the international level, but
information on such sharing is not necessarily
reported by individual countries.
On an annual basis, countries report to UNODC
on key activities related to international cooperation
in the field of drug supply, including on joint opera-
tions with other countries, controlled deliveries,
exchanges of liaison officers and the exchange of
information. The reporting includes information
on whether such activities took place during the
reference year. In most countries and at the inter-
national level, no information is collected to assess
the actual quality or the effectiveness of such coop-
eration activities.
While the proportion of countries that at least par-
tially complete the section on international
cooperation in their annual data submissions is quite
high (close to 100 per cent of all countries report-
ing information to UNODC), a significant number
of countries do not submit any information on inter-
national cooperation to UNODC; for example, out
INTERNATIONAL
COOPERATION
It is generally acknowledged that the drug problem
is not restricted to just one country, but that it affects
most countries in an intertwined manner. Responses
to the drug problem at the national level are neces-
sary, but they are not sufficient to cope with the
global drug problem unless they are also well coor-
dinated across countries. For example, interventions
in one country, leading to a reduction in the drug
supply, may prompt a replacement effect, with
supply increasingly originating in other countries.
Similarly, successful demand reduction efforts in
just one country may prompt organized crime
groups to devise strategies for targeting other coun-
tries and trigger increasing demand for drugs at the
regional or global level. In short, global drug markets
tend to be extremely resilient to attempts to solve
the drug problem exclusively at the national level.
One of the key approaches to addressing the trans-
national nature of the drug problem has been the
strengthening of international cooperation, both
with a view to improving coordination of policies
and interventions and assisting countries with lim-
ited resources and capacities in undertaking the
necessary interventions. International cooperation
can take many forms, including intergovernmental
cooperation frameworks and mechanisms, the devel-
opment of standards and guidelines that promote
best practices in the fields of drug demand reduc-
tion
52
or drug supply reduction, and capacity-building
initiatives that strengthen the ability of countries to
counter the drug problem.
A comprehensive analysis of international coopera-
tion on drug-related issues, which may be
implemented at different levels, whether geographi-
cally or thematically, involving a plurality of
mechanisms and actors – even if only done concep-
tually – would go far beyond the scope of this
edition of the World Drug Report. Nonetheless, this
broad range of international cooperation activities
52 See, for example, UNODC and WHO, International
Standards on Drug Use Prevention, second updated edition
(Vienna, 2018); UNESCO, UNODC and WHO, Good
Policy and Practice in Health Education: Booklet 10 – Educa-
tion Sector Responses to the Use of Alcohol, Tobacco and Drugs
(Paris, 2017).

Interpreting reported data on international cooperation by
Member States
Member States report to UNODC on international
cooperation through the annual report questionnaire.
However, replies to the questions on international coop-
eration were only received by around 40 per cent of the
countries that were invited to complete the annual
report questionnaire over the period 2017–2018. Euro-
pean countries, which usually report high levels of cross-
border cooperation, are overrepresented in this sample
(61 per cent of all European countries reported on
international cooperation), while other regions (notably
Africa and Oceania) are underrepresented. This limits
the interpretation of the global data received, as they
may be skewed by a reporting bias towards regions with
a high capacity to engage in international cooperation.
The main unknown is whether and to what extent non-
reporting countries, if they had reported, would have
provided similar answers to questions on international
cooperation as those reporting. While this cannot be
known unless a specific study of non-respondents is car-
ried out, it is most likely that the actual proportion of
countries involved in cross-border cooperation falls
within a range between (a) the number of countries
reporting specific cross-border cooperation activities,
expressed as the proportion of all countries that received
the annual report questionnaire (constituting the abso-
lute minimum); and (b) the number of countries report-
ing specific cross-border cooperation activities, expressed
as the proportion of the countries responding either
affirmatively or negatively to questions on whether or
not they had carried out such specific cross-border oper-
ation activities. The latter is based on the hypothesis
that non-reporting countries would show similar pat-
terns of international cooperation as those reporting,
which probably constitutes the maximum. In fact, it
seems highly unlikely that non-reporting countries
would, on average, be more involved in international
cooperation than reporting countries, as the latter are
more often located in regions, such as Europe, where the
capacity to engage in international cooperation is likely
bigger and the framework for such cooperation is more
institutionalized.
For these reasons, the analyses of responses to the annual
report questionnaire in this chapter are presented in
ranges based on proportion (a) and proportion (b) men-
tioned above. While these ranges may sometimes be
wide, one should refrain from calculating mid-points, as
they would be misleading, in particular because in most
cases it is likely that the actual proportions would still
be closer to proportion (b) than to the absolute mini-
mum, proportion (a).
23
International cooperation
6
Number of countries providing data on international cooperation in the annual report question-
naire and their proportion among countries that received the annual report questionnaire, by
region, 2017–2018
Source: UNODC, responses to the annual report questionnaire.
Note: For the purposes of these calculations, a country was considered to have reported on international cooperation if it had provided informa-
tion on whether it had engaged or not engaged in at least one of the following activities: joint operations, controlled deliveries, the exchange of
liaison officers, the exchange of information or the extradition of drug traffickers, in either 2017 or 2018.
77
28
20
13
14
2
39%
61%
41%
36%
27%
14%
0%
10%
20%
30%
40%
50%
60%
70%
80%
0
10
20
30
40
50
60
70
80
Global Europe Asia Americas Africa Oceania
Proportion of reporting countries
in region (percentage)
Number of reporting countries in region
Number of reporting
countries
Proportion of reporting
countries in region
77
28
20
13
14
2
39%
61%
41%
36%
27%
14%
0%
10%
20%
30%
40%
50%
60%
70%
80%
0
10
20
30
40
50
60
70
80
Global Europe Asia Americas Africa Oceania
Proportion of reporting countries
in region (percentage)
Number of reporting countries in region
Number of reporting
countries
Proportion of reporting
countries in region
77
28
20
13
14
2
39%
61%
41%
36%
27%
14%
0%
10%
20%
30%
40%
50%
60%
70%
80%
0
10
20
30
40
50
60
70
80
Global Europe Asia Americas Africa Oceania
Proportion of reporting countries
in region (percentage)
Number of reporting countries in region
Number of reporting
countries
Proportion of reporting
countries in region

24
2010–2018. This is quite a broad range, leaving the
door wide open to interpretations as to the impor-
tance of joint operations between law enforcement
across countries.
In 2018, seven countries, mostly located in Africa
and, to a lesser extent, in South and Central Amer-
ica, reported no joint operations, while 59
countries, mostly located in Europe (24 countries),
followed by Asia (15), the Americas (10), Africa
(8) and Oceania (2), were involved in joint cross-
border operations.
The involvement of law enforcement in joint opera-
tions among countries providing such information
throughout the period 2010–2018 appears to have
declined slightly in recent years, falling – if only
International cooperation has been at the heart of international
drug control for more than a century
The strengthening of international cooperation has
been at the heart of international drug control since the
convening of the Shanghai Opium Commission in
1909. That was followed by the first International
Opium Convention, signed at the Hague in 1912, the
three drug conventions of the League of Nations (1925,
1931, 1936) and the three drug conventions adopted by
the United Nations (1961, 1971 and 1988).
International cooperation continued to play a key role
in more recent policy documents. The Political Declara-
tion and Plan of Action on International Cooperation
towards an Integrated and Balanced Strategy to Counter
the World Drug Problem, adopted during the high-level
segment of the fifty-second session of the Commission
on Narcotic Drugs, in 2009,
a
makes multiple mentions,
32 in all, of the need for more and better international
cooperation, putting it on par with other strategies
referred to in the Political Declaration, such as demand
and supply reduction.
b
a See, for example, paragraph 1 of the Political Declaration: “We,
the States Members of the United Nations … 1. Reaffirm our
unwavering commitment to ensure that all aspects of demand
reduction, supply reduction and international cooperation are
addressed…” (E/2009/28, chap. I, sect. C (Political Declaration,
para. 1)).
Similarly, in the outcome document of the special ses-
sion of the General Assembly held in 2016, entitled
“Our joint commitment to effectively addressing and
countering the world drug problem”, the need to
enhance and increase cooperation to face the various
challenges linked to the drug problem, including the
need to increase and strengthen international coopera-
tion, is explicitly mentioned multiple times.
c
Lastly, the 2019 Ministerial Declaration on “Strength-
ening Our Actions at the National, Regional and Inter-
national Levels to Accelerate the Implementation of
Our Joint Commitments to Address and Counter the
World Drug Problem” committed to further strengthen-
ing cooperation and coordination among national
authorities, particularly in the health, education, social,
justice and law enforcement sectors, and between gov-
ernmental agencies and other relevant stakeholders,
including the private sector, at all levels, including
through technical assistance; as well as to strengthening
bilateral, regional and international cooperation and
promoting information-sharing.
b
See Official Records of the Economic and Social Council, 2009,
Supplement No. 8 (E/2009/28), chap. I, sect. C.
c
General Assembly resolution S-30/1, annex.
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
of an average of 196 annual report questionnaires
sent out every year, 72 countries provided replies
on the issue in 2018, while 124 countries and ter-
ritories did not. This reporting rate limits
interpretation of the information reported to
UNODC for any specific year, and also limits the
ability to make comparisons over time, since the
countries that provide replies change from year to
year.
Joint cross-border drug operations
Data show that an average of 67 countries, i.e., 35
per cent of all countries to which the questionnaires
were sent (196 countries), or 90 per cent of coun-
tries that actually reported, were involved in joint
cross-border drug operations over the period

25
International cooperation
6
Fig. 12
International cross-border cooperation, 2010–2018
Source: E/CN.7/2020/6.
Note: This analysis is based on 196 countries to which the annual report questionnaire is sent every year and on information provided by 75
countries that reported throughout the period 2010–2018 (by either providing an answer to each question or leaving the answer blank).
The percentages represent the proportion of countries reporting their involvement in each activity for each biennium out of all countries
providing such information (i.e. countries reporting either “yes” or “no” to the respective question asked).
Fig. 13
Countries reporting joint cross-border operations, 2010–2018
Source: UNODC, responses to the annual report questionnaire.
99%
95%
94%
91%
92%
94%
93%
89%
91%
95%
77%
74%
79%
72%
77%
100%
100%
100%
100%
100%
0
20
40
60
80
100
120
140
160
180
200
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
Joint operations with other
countries
Controlled delivery Exchange of liaison officers Exchange of
information
Number of countries
Yes
No
No response to question
Part II of questionnaire not submitted for all bienniums
countries reporting throughout the period 2010–
2018 are considered – from 68 countries in the
period 2010–2011 to 57 in the period 2017–2018.
The reasons for this downward trend in joint opera-
tions in recent years are unknown. It can be
speculated that among the multiple causes, the
budgetary problems following the 2008 financial
crisis may have played a role. Moreover, over the
years, Member States have reported that they have
faced a number of challenges in joint operations,
which may also have contributed to the decrease.
These challenges include “slow formal procedures”
67
8
0
10
20
30
40
50
60
70
80
2010
2011
2012
2013
2014
2015
2016
2017
2018
Average,
2010 ̶ 2018
Number of countries
Average number of countries
reporting no participation in joint
operations with other countries
Average number of countries
reporting participation in joint
operations with other countries
Countries reporting participation in
joint operations with other countries
Countries reporting no participation
in joint operations with other
countries
67
8
0
10
20
30
40
50
60
70
80
2010
2011
2012
2013
2014
2015
2016
2017
2018
Average,
2010 ̶ 2018
Number of countries
Average number of countries
reporting no participation in joint
operations with other countries
Average number of countries
reporting participation in joint
operations with other countries
Countries reporting participation in
joint operations with other countries
Countries reporting no participation
in joint operations with other
countries

26
Controlled deliveries
Article 1 of the 1988 Convention against Illicit Traffic
in Narcotic Drugs and Psychotropic Substances defines
controlled delivery as a “technique of allowing illicit or
suspect consignments of narcotic drugs, psychotropic
substances, substances in Table I and Table II annexed
to this Convention, or substances substituted for them,
to pass out of, through or into the territory of one or
more countries, with the knowledge and under the
supervision of their competent authorities, with a view
to identifying persons involved in the commission of
offences established in accordance with article 3, para-
graph 1, of the Convention”. Article 11 is then fully
dedicated to this technique, asking all parties to the
Convention to take all the necessary measures “to allow
for the appropriate use of controlled delivery at the
international level”. The technique of controlled deliv-
ery was also advocated in subsequent international drug
policy instruments, including the 2009 Political Decla-
ration and Plan of Action.
OTHER DRUG POLICY ISSUES
providing a reply to the question on controlled deliv-
ery over the period 2010–2018. Some fluctuations
but no clear trend in the number of countries report-
ing controlled deliveries can be identified over the
period 2010–2018. In 2018, a total of 64 countries
reported having been involved in at least one con-
trolled delivery, including 26 countries located in
Europe (mostly in Western and Central Europe),
16 in Asia, 11 in the Americas (mostly in Latin
America and the Caribbean), 9 in Africa and 2 in
Oceania. The five countries reporting no participa-
tion in controlled deliveries were all located outside
Europe: three in Africa and one each in the Carib-
bean and South-East Asia.
While few law enforcement specialists would be likely
to question the inherent merits of controlled deliv-
eries of drugs, information provided by countries to
UNODC suggests that they do not necessarily form
part of the tasks expected of law enforcement author-
ities in several countries. Controlled deliveries require
long-lasting partnerships among national agencies,
connections that can easily be activated when coop-
eration on ongoing operations is needed quickly.
They can also be resource-intensive; and where they
are not included among the success indicators of
national law enforcement agencies, the incentive for
national agencies to engage in controlled delivery
operations may be limited.
Exchange of liaison officers
Another example of cross-border cooperation is the
exchange of liaison officers, which facilitates the
informal exchange of information between
(37 countries over the period 2017–2018), “lack of
agreements enabling operational cooperation” (15
countries), “inability to identify appropriate coun-
terparts” (14 countries) and problems related to the
“lack of a common language” practiced and under-
stood by law enforcement officials from different
countries (11 countries). Paradoxically, however,
reported data also suggest that such obstacles to
successful international cooperation decreased
slightly in importance between the periods 2010–
2011 and 2017–2018.
53
Controlled deliveries of drugs
The active participation of national law enforcement
agencies in controlled deliveries of drugs is another
important area of international cooperation. Such
measures typically target complex and long-lasting
operations and are aimed at dismantling transna-
tional drug trafficking networks operating across
countries. They do not focus on couriers who handle
small quantities of drugs and the seizing of small
quantities of drugs, but rather attempt to dismantle
whole networks operating across countries.
On average, 69 countries per year acknowledged
their involvement in controlled deliveries of drug
shipments over the period 2010–2018, representing
36 per cent of all countries receiving the annual
report questionnaire and 86 per cent of all countries
53 Report of the Executive Director on action taken by
Member States to implement the Political Declaration and
Plan of Action on International Cooperation towards an
Integrated and Balanced Strategy to Counter the World
Drug Problem (E/CN.7/2020/6).
WORLD DRUG REPORT 2020

27
International cooperation
6
countries and thus creates an environment of more
timely and effective cooperation. There are cases in
which liaison officers, with the help of their net-
works, were able to prevent drug shipments from
leaving the countries where they were stationed,
instead of having to wait until the drugs arrived in
the countries of final destination, which could
increase the risk of some of the drugs being diverted
to other destinations before being seized in the
countries of final destination.
However, it remains difficult to evaluate to what
extent improved international cooperation, includ-
ing the exchange of liaison officers, may have
contributed to the increase in the last two decades
of the quantities of drugs intercepted in source and
transit countries.
54
No clear trend in the number of countries reporting
the exchange of liaison officers can be identified
over the period 2010–2018, when an average of 57
countries reported the exchange of liaison officers.
It is likely that the proportion of countries exchang-
ing liaison officers falls within a broad range of
between 29 per cent of all countries to which the
questionnaire was sent and 74 per cent of all report-
ing countries over the period 2010–2018.
In 2018, 52 countries reported the exchange of liai-
son officers, most of which were located in Europe
(20), followed by Asia (12), the Americas (9), Africa
54 UNODC, responses to the annual report questionnaire.
(9) and Oceania (2). By comparison, 14 countries,
located across all regions, reported having had no
exchange of liaison officers in 2018.
However, the number of countries reporting on an
“information exchange via liaison officers” was actu-
ally larger (62 countries over the period 2010–2018,
or 66 countries in 2018), suggesting that not all
countries where foreign liaison officers were actually
stationed reported having been involved in the
exchange of liaison officers. Combining the responses
to the two questions on involvement in the exchange
of liaison officers and information exchange with
liaison officers actually reveals that a total of 68 coun-
tries (35 per cent of all the countries to which the
annual report questionnaire was sent) appear to have
had links with liaison officers in 2018. This includes
27 countries in Europe, 16 in Asia, 13 in the Ameri-
cas, 10 in Africa and 2 in Oceania.
Exchange of information
All reporting countries seem to engage in the
exchange of information with appropriate counter-
parts in other countries and/or with international
organizations. On average, 82 countries reported
having exchanged information on drug-related issues
with other countries over the period 2010–2018
(42 per cent of all countries to which the question-
naires were sent, or more than 99 per cent of all
reporting countries).
55
In 2018, only two countries
55 E/CN.7/2020/6.
Fig. 14
Countries reporting controlled deliveries of drugs, 2010–2018
Source: UNODC, responses to the annual report questionnaire.
69
9
0
10
20
30
40
50
60
70
80
2010 2012 2014 2016 2018 Average,
2010 ̶
2018
Number of countries
Average number of countries
reporting no participation in
controlled deliveries
Average number of countries
reporting participation in controlled
deliveries
Countries reporting participation in
controlled deliveries
Countries reporting no participation
in controlled deliveries
69
9
0
10
20
30
40
50
60
70
80
2010 2012 2014 2016 2018 Average,
2010 ̶
2018
Number of countries
Average number of countries
reporting no participation in
controlled deliveries
Average number of countries
reporting participation in controlled
deliveries
Countries reporting participation in
controlled deliveries
Countries reporting no participation
in controlled deliveries

28
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
reported no information exchange (one in sub-Saha-
ran Africa and one in Latin America), while 70
countries reported having exchanged information
on drug-related issues, most notably countries in
Europe (26), followed by countries in Asia (17),
Africa (13), the Americas (12) and Oceania (2).
56
The exchange of information was mostly undertaken
in the context of international meetings (64 coun-
tries on average over the period 2010–2018), direct
communication (64 countries) and information
exchange through INTERPOL (64 countries), fol-
lowed by information exchange through liaison
officers (62 countries), information exchange
through regional organizations (58 countries), dip-
lomatic channels (52 countries) and information
exchange through the World Customs Organization
(48 countries).
57
Extradition of drug law offenders
One of the specific results of international judicial
cooperation is the extradition of drug law offenders.
This measure was originally agreed in the Single
Convention on Narcotic Drugs of 1961
58
and has
been high on the international agenda ever since the
adoption of the United Nations Convention against
Illicit Traffic in Narcotic Drugs and Psychotropic
56 UNODC, responses to the annual report questionnaire.
57 E/CN.7/2020/6.
58 See article 36.
Substances of 1988,
59
as well as the 2009 Political
Declaration and Plan of Action.
60
The number of countries reporting the extradition
of drug law offenders has fluctuated over the past
decade. On average, 34 countries per year reported
such extraditions over the period 2010–2018, which
is equivalent to 18 per cent of all countries that
received the questionnaire or 49 per cent of all
reporting countries. Extraditions of drug law offend-
ers thus seem to be less widespread globally than
other forms of international cooperation. Most of
the countries that reported the extradition of drug
law offenders over the period 2010–2018 were
located in Europe (an average of 17 countries per
year), followed by the Americas (10 countries,
mostly in Latin America and the Caribbean), Africa
and the Middle East (4 countries) and Asia and
Oceania (3 countries). By comparison, most of the
countries that had not extradited drug law offend-
ers (an average of 35 countries per year over the
period 2010–2018) were located in Asia and Oce-
ania (12 countries) and in Africa and the Middle
East (10 countries).
The reasons why some countries extradite more than
others are not clear. There are, of course, differences
in the numbers of foreign drug traffickers arrested
who are potentially subject to extradition. Moreover,
59 See article 6.
60 See E/2009/28.
Fig. 15
Countries reporting exchange of liaison officers, 2010–2018
Source: UNODC, responses to the annual report questionnaire.
57
20
0
10
20
30
40
50
60
70
80
2010
2011
2012
2013
2014
2015
2016
2017
2018
Average,
2010 ̶ 2018
Number of countries
Average number of countries
reporting no participation in joint
operations with other countries
Average number of countries
reporting participation in joint
operations with other countries
Countries reporting participation
in joint operations with other
countries
Countries reporting no
participation in joint operations
with other countries
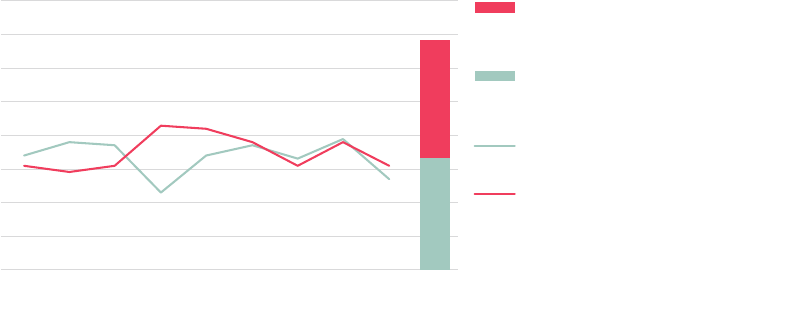
29
International cooperation
6
extradition treaties between countries provide the
basis for extraditions and play a key role. In addi-
tion, differences in extradition policies may have an
impact on the readiness of countries to extradite
drug law offenders. In this regard, the application
of the death penalty for drug law offences may also
limit extraditions.
International technical cooperation
International technical cooperation in drug supply
reduction efforts encompasses the receipt of assis-
tance in such efforts from another country or from
an international organization in the form of train-
ing, the provision of software (e.g., for processing
border control information), financial assistance or
assistance in data sharing, as well as the provision
of such assistance to other countries.
The number of countries receiving such technical
assistance appears to have increased slightly over the
period 2010–2018, while the number of countries
providing such assistance, although fluctuating,
appears to have remained rather stable. Overall, 56
countries reported having obtained technical assis-
tance in the area of drug supply reduction in 2018,
up from 50 countries in 2010. By comparison, the
number of countries that provided technical assis-
tance to other countries in the area of drug supply
reduction amounted to 37 countries in 2018, almost
unchanged since 2010.
Most of the technical assistance provided to other
countries in the area of drug supply reduction in
2018 appears to have been in the form of training
(30 countries), financial assistance (12 countries),
equipment (10 countries) and software (10
countries).
61
This mirrors the most common forms
of assistance reported to have been received – train-
ing and assistance in data sharing, followed by the
provision of equipment and software.
62
The assistance received was judged sufficient for
their needs by most reporting countries in Europe
(88 per cent in the period 2017–2018) and in Asia
and Oceania (58 per cent). By contrast, in Africa
and the Americas, only a minority of reporting coun-
tries regarded the assistance received as meeting their
needs (40 and 43 per cent, respectively).
63
Development assistance
dedicated to drug control
has declined
Donor countries report to the Development Assis-
tance Committee (DAC) of OECD on areas in
which they have committed themselves to providing
funds for development assistance or have actually
disbursed such funds to support developing coun-
tries. The reported statistics primarily include
61 UNODC, responses to the anual response questionnaire.
62 E/CN.7/2020/6.
63 Ibid.
Fig. 16
Countries reporting extraditions of drug law offenders, 2010–2018
Source: UNODC, responses to the annual report questionnaire.
34
35
0
10
20
30
40
50
60
70
80
2010
2011
2012
2013
2014
2015
2016
2017
2018
Average,
2010 ̶ 2018
Number of countries
Average number of countries
reporting no extraditions of drug
offenders
Average number of countries
reporting extraditions of drug
offenders
Number of countries reporting
extraditions of drug offenders
Number of countries reporting no
extraditions of drug offenders
34
35
0
10
20
30
40
50
60
70
80
2010
2011
2012
2013
2014
2015
2016
2017
2018
Average,
2010 ̶ 2018
Number of countries
Average number of countries
reporting no extraditions of drug
offenders
Average number of countries
reporting extraditions of drug
offenders
Number of countries reporting
extraditions of drug offenders
Number of countries reporting no
extraditions of drug offenders

30
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
information on funds provided by the 30 members
of DAC, all of which are OECD members. Moreo-
ver, they include information provided by a number
of European OECD member countries that are not
DAC members (mostly countries in South-Eastern
Europe and the Baltic area), as well as a number of
other non-DAC-member donor countries (mostly
oil- and gas-producing countries, such as most of
the Gulf countries, the Russian Federation, Kazakh
-
stan and Azerbaijan, as well as a few other countries
in Asia, such as Israel and Thailand). Funds provided
to developing countries by multilateral bodies, such
as the United Nations, the European Union, the
International Monetary Fund, the World Bank and
the various regional development banks, are also
included. Funds provided by other emerging donor
countries, such as China, seem not to be included
in these statistics.
64
The statistics are provided both in terms of com-
mitments made by donor countries and in terms of
64 OECD, “Query Wizard for International Development Sta-
tistics”.
actual gross disbursements related to drug control.
In most years, the former has tended to be higher
than the latter. In any case, DAC statistics show a
two-and-a-half-fold increase in development assis-
tance by donor countries over the period 2000–2017,
expressed in constant United States dollars, both in
terms of overall commitments made and gross dis-
bursements of development aid.
By contrast, commitments and disbursements dedi-
cated explicitly to drug control fell by 98 and 89
per cent, respectively, over that period. Most of the
decline was reported over the period 2006–2010,
followed by a stabilization at low levels ever since.
Expressed as a proportion of total development aid,
drug control-related commitments fell from a pro-
portion of 3 per cent of all development assistance
in 2000 to 0.02 per cent in 2017. In parallel, gross
disbursements related to drug control fell from 1.9
per cent of all such disbursements for development
assistance in 2003 to 0.04 per cent in 2017.
65
65 OECD, OECD.Stat, Development, Flows based on indi-
vidual projects, “Creditor Reporting System (CRS)”.
Fig. 17
Countries reporting having received or provided technical assistance in the area of drug
supply reduction during the reporting year, 2010–2018
Source: UNODC, responses to the annual report questionnaire.
56
20
36
33
0
20
40
60
80
2010 2011 2012 2013 2014 2015 2016 2017 2018 Received
or not
Provided
or not
Technical
assistance
Average,
2010 ̶ 2018
Number of countries
Technical assistance not provided: average 2010 ̶ 2018
Technical assistance provided: average 2010 ̶ 2018
Technical assistance not received: average 2010 ̶ 2018
Technical assistance received: average 2010 ̶ 2018
Technical assistance received
Technical assistance not received
Technical assistance provided
Technical assistance not provided
56
20
36
33
0
20
40
60
80
2010 2011 2012 2013 2014 2015 2016 2017 2018 Received
or not
Provided
or not
Technical
assistance
Average,
2010 ̶ 2018
Number of countries
Technical assistance not provided: average 2010 ̶ 2018
Technical assistance provided: average 2010 ̶ 2018
Technical assistance not received: average 2010 ̶ 2018
Technical assistance received: average 2010 ̶ 2018
Technical assistance received
Technical assistance not received
Technical assistance provided
Technical assistance not provided
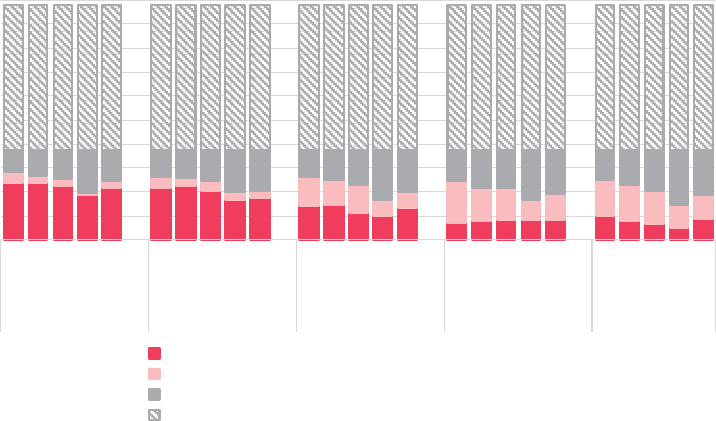
31
International cooperation
6
Without more detailed information, it is difficult
to judge to what extent the massive declines shown
in these data reflect real declines in funds provided
for drug control purposes, or whether they only
reflect some changes in accounting practices. Some
countries such as Colombia and Peru have become
less reliant on donor assistance for drug control, but
it cannot be excluded that Member States may
simply provide development assistance under other
budget lines.
Most assistance for drug control is
provided to the Americas and Asia
The primary recipients of overall development assis-
tance over the period 2002–2017 were countries in
Africa and in Asia, with little change between the
periods 2002–2009 and 2010–2017.
66
By contrast, development assistance dedicated exclu-
sively to drug control purposes was dominated by
funds made available primarily to countries in the
Americas, in particular over the period 2002–2009
66 Ibid.
(67 per cent of the global total), followed by Asia.
The latter became the main receiving region over
the period 2010–2017 period (48 per cent of the
global total), followed by the Americas (23 per cent
of the global total). Assistance to those regions likely
reflects the concentration of cocaine production and
trafficking in the Americas and opium and heroin
production and trafficking in Asia. The funds made
available to Africa increased from 0.3 per cent of
the global total over the period 2002–2009 to 8 per
cent of the global total over the period 2010–2017,
reflecting the emerging importance of drug traffick-
ing and use in Africa.
67
At the same time, OECD data point to a significant
reduction in funds made available by donor coun-
tries for drug control purposes, from an average of
$1.1 billion per year over the period 2002–2009
to $77 million per year over the period 2010–
2017.
68
This contrasts with the continued calls for
more international cooperation on drug control
67 Ibid.
68 Ibid.
Fig. 18
Member States that received technical assistance in the area of drug supply reduction, by
type of assistance, 2010–2018
Source: E/CN.7/2020/6.
Note: This analysis is based on 196 countries to which the annual report questionnaire is sent every year and on information provided by
75 countries that reported throughout the period 2010–2018 (by either providing an answer to each question or leaving the answer
blank). The percentages represent the proportion of countries reporting their involvement in each activity for each biennium out of all
countries providing such information (i.e. countries reporting either “yes” or “no” to the respective question asked).
86%
89%
88%
95%
88%
81%
87%
84%
83%
85%
53%
58%
50%
61%
65%
29%
37%
40%
52%
45%
40%
35%
32%
34%
49%
0
20
40
60
80
100
120
140
160
180
200
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
2010 ̶ 11
2012 ̶ 13
2014 ̶ 15
2016
2017 ̶ 18
Training Data sharing Equipment Financial Software
Number of countries
Yes
No
No response to question
Part II of questionnaire not submitted for all bienniums

32
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
issues and more funding of such activities. Such
marked declines affected all regions, in particular
the Americas.
The net increase in overall development assistance
over the past two decades (from $112 billion to $159
billion per year),
69
makes it difficult, however, to
assess to what extent the reported declines in funds
made available for drug control purposes were merely
statistical artefacts, possibly offset by additional funds
made available under different budget lines.
As reflected in the OECD statistics on gross dis-
bursement of development assistance, the single
largest recipient of development assistance related
to drug control, excluding funds made available for
alternative development, over the period 2002–2017
was Colombia ($3.7 billion, expressed in 2017
United States dollars), followed by Afghanistan ($1.3
billion), Peru ($0.6 billion), the Plurinational State
69 Ibid.
of Bolivia ($0.5 billion), Pakistan ($0.3 billion),
Ecuador ($0.3 billion) and Mexico ($0.2 billion),
that is, all the countries affected by significant illicit
drug production and/or drug trafficking activities.
Most of those countries saw significant reductions
in drug-related funding of development assistance
between the periods 2002–2009 and 2010–2017.
At the same time, several of those countries still
benefited from an overall increase in development
assistance over the two periods, including Colombia,
Bolivia (Plurinational State of ) and Mexico in the
Americas and Afghanistan and Pakistan in Asia.
70
However, UNODC is also aware that several coun-
tries mentioned above have integrated a number of
drug control activities into their national budgets
in recent years. Such activities were previously sup-
ported by the international community, thus often
rendering direct comparisons difficult.
70 Ibid.
Fig. 19
Commitments and disbursement of funds by donor countries reporting to the Development
Assistance Committee on development assistance in general and development assistance
dedicated to drug control, 2000–2017
Source: OECD, OECD.Stat, Development, Flows based on individual projects, “Creditor Reporting System (CRS)”.
Note: The statistics include information provided by observers of international institutions such as the United Nations Development Pro-
gramme, the World Bank, the International Monetary Fund and various regional development banks, as well as by other OECD member
countries and non-OECD-member DAC “participants”, including several oil-producing countries, such as Gulf States, the Russian Federation,
Kazakhstan and Azerbaijan.
0
1,000
2,000
3,000
4,000
0
50,000
100,000
150,000
200,000
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
Development assistance related to drug
control (millions of constant 2017 dollars)
All development assistance
(millions of constant 2017 dollars)
All development assistance ̶ commitments
All development assistance ̶̶ disbursements
Development assistance related to drug control ̶ commitments
Development assistance related to drug control ̶ disbursements
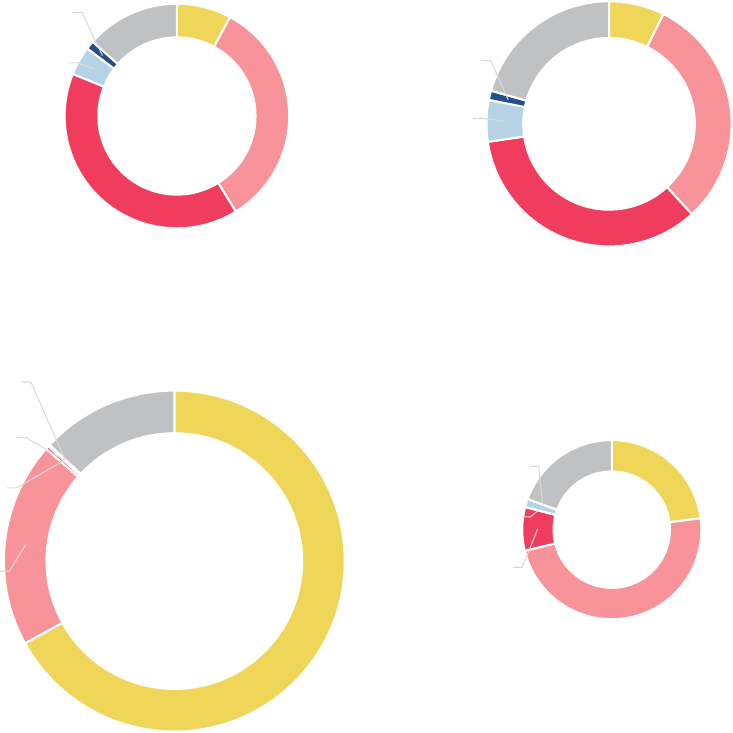
33
International cooperation
6
Most funds are sourced from the
United States and the European Union
Regarding the origin of development funds made
available for the purposes of drug control, DAC
statistics suggest that, over the period 2002–2017,
most such funds were provided by the United States,
followed by the European Union (including its
Available data also suggest that the overall lesser
funds available for drug control from development
assistance are now shared between more beneficiary
countries, rising from an average of 47 countries per
year over the period 2002–2009 to 69 countries
over the period 2010–2017 (82 countries in 2017).
71
71 Ibid.
Fig. 20
Regional distribution of gross disbursements of all development assistance and of drug
control-related assistance, 2002–2009 and 2010–2017
Source: OECD, OECD.Stat, Development, Flows based on individual projects, “Creditor Reporting System (CRS)”.
2002–2009
All development assistance
(N = $112 billion per year in constant 2017 dollars)
2010–2017
All development assistance
(N = $159 billion per year in constant 2017 dollars)
2002–2009
Drug control-related development assistance
(N = $1.093 billion per year in constant 2017 dollars)
2010–2017
Drug control-related development assistance
(N = $77 million per year in constant 2017 dollars)
Americas
8%
Asia
33%
Africa
40%
Europe
4%
Oceania
1%
Non-defined
14%
Americas
67%
Asia
20%
Africa
0.3%
Europe
0.2%
Oceania
0.01%
Non-defined
13%
Americas
23%
Asia
48%
Africa
8%
Europe
2%
Oceania
0%
Non-defined
19%
Americas
7%
Asia
31%
Africa
34%
Europe
6%
Oceania
1%
Non-defined
21%
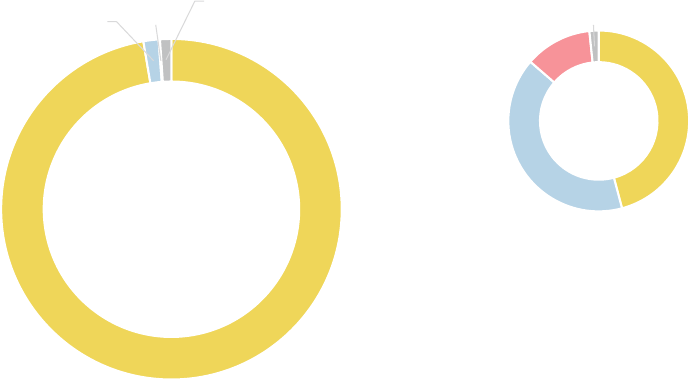
34
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
member States) and Japan. Although the share pro-
vided by the United States continues to be the largest
worldwide, the shares provided by both the Euro-
pean Union (and its member States) and Japan
increased over the period 2010–2017, as compared
with the period 2002–2009.
Development assistance dedicated to
drug control has started to show an
upward trend again in recent years
Irrespective of the clear long-term downward trend
in assistance provided to developing countries for
drug control purposes, there have again been signs
of an upward trend in recent years (2015–2017)
with regard to both commitments and gross dis-
bursements of funds for drug control-related
activities. At the same time, data also suggest that,
even at current growth rates, it will nevertheless take
a long time for the levels of funds dedicated to drug
control that were available at the beginning of the
new millennium to be reached again.
Has international cooperation
led to global quantities of
drugs seized growing faster
than global drug production?
The quantities of drugs seized have clearly increased
over the past decades. This could be the consequence
of more drugs being smuggled and/or of improved
law enforcement efforts. If the growth in the volume
of drugs seized outpaces the growth in the volume
produced, however, it can be assumed that interdic-
tion capabilities have effectively improved. This is
reflected in available data: while cocaine manufac-
ture at the global level doubled over the period
1998–2018, the quantity of cocaine seized globally
more than tripled. Likewise, global opium produc-
tion rose by around 80 per cent over the period
1998–2018, while the quantity of opiates seized
globally tripled.
Even when taking into account the possibility that
changes in drug seizures may not be fully comparable
with changes in drug production, because seizures
are reported in terms of heterogeneous purity levels
Fig. 21
Donors of development assistance funds dedicated to drug control, 2002–2017
Source: OECD, OECD.Stat, Development, Flows based on individual projects, “Creditor Reporting System (CRS)”.
2002–2009
(N = $1.093 billion per year in constant 2017 dollars)
2010–2017
(N = $77 million per year in constant 2017 dollars)
United States
97%
European Union and
European Union
member States
2%
Japan
0.1%
Other
1.1%
United States
46%
European Union and
European Union
member States
40%
Japan
12.0%
Other
1.7%
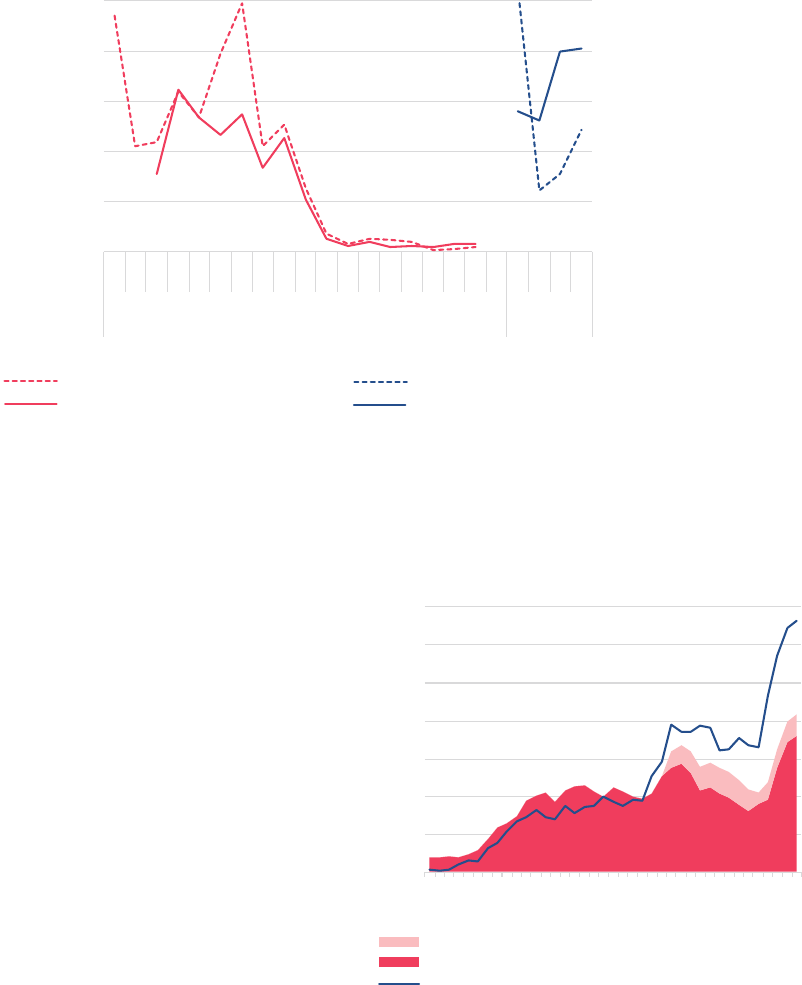
35
International cooperation
6
while production is estimated in terms of fixed purity
levels, the fact that seizures have increased far more
than production – with no indications of massive
declines in the purity levels of drugs trafficked at the
global level – suggests that rates of global drug inter-
diction have increased over the years. It is likely that
a number of the largest drug seizures, which con
-
tributed to these results, would not have been
possible without international cooperation.
The link between expenditure on drug control by
donor countries as part of their development assis-
tance and the results of related international
cooperation in terms of law enforcement successes
in seizing drugs is not at all clear, and all attempts
to provide an explanation remain highly speculative.
One possible explanation could be that the large
amount of funds dedicated to drug control at the
beginning of the new millennium may have con-
tributed to improved cooperation on drug control
issues at the global level and across countries. Once
this cooperation became institutionalized, it con-
tinued, even though it appears that far smaller
amounts of new funds were made available by the
international community over the past decade.
Fig. 22
Commitments and disbursements of development assistance funds for drug control:
long-term trends versus short-term trends
Source: OECD, OECD.Stat, Development, Flows based on individual projects, “Creditor Reporting System (CRS)”.
0
20
40
60
80
100
0
500
1,000
1,500
2,000
2,500
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2014
2015
2016
2017
Long-term trends Short-term
trends
Short-term trends
(millions of constant 2017 dollars)
Long-term trends
(millions of constant 2017 dollars)
Commitments ̶ long-term trends Disbursements ̶ long-term trends
Commitments ̶ short-term trends Disbursements ̶ short-term trends
0
20
40
60
80
100
0
500
1,000
1,500
2,000
2,500
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2014
2015
2016
2017
Long-term trends Short-term
trends
Short-term trends
(millions of constant 2017 dollars)
Long-term trends
(millions of constant 2017 dollars)
Commitments ̶ long-term trends Disbursements ̶ long-term trends
Commitments ̶ short-term trends Disbursements ̶ short-term trends
0
20
40
60
80
100
0
500
1,000
1,500
2,000
2,500
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2014
2015
2016
2017
Long-term trends Short-term
trends
Short-term trends
(millions of constant 2017 dollars)
Long-term trends
(millions of constant 2017 dollars)
Commitments ̶ long-term trends
Disbursements ̶ long-term trends
Commitments ̶ short-term trends Disbursements ̶ short-term trends
0
20
40
60
80
100
0
500
1,000
1,500
2,000
2,500
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2014
2015
2016
2017
Long-term trends Short-term
trends
Short-term trends
(millions of constant 2017 dollars)
Long-term trends
(millions of constant 2017 dollars)
Commitments ̶ long-term trends Disbursements ̶ long-term trends
Commitments ̶ short-term trends Disbursements ̶ short-term trends
0
20
40
60
80
100
0
500
1,000
1,500
2,000
2,500
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2014
2015
2016
2017
Long-term trends Short-term
trends
Short-term trends
(millions of constant 2017 dollars)
Long-term trends
(millions of constant 2017 dollars)
Commitments ̶ long-term trends Disbursements ̶ long-term trends
Commitments ̶ short-term trends Disbursements ̶ short-term trends
Fig. 23
Growth in global cocaine manufacture and
global quantities of cocaine seized, 1980–
2018
Sources: UNODC, responses to the annual report questionnaire (for
data on seizures); UNODC coca cultivation surveys; and United States,
Department of State, International Narcotics Control Strategy
Reports (for cocaine manufacture estimates).
Note: The 2018 estimates of cocaine manufacture are provisional.
0
50
100
150
200
250
300
350
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
Index: 1998 = 100
Cocaine manufacture ̶ new conversion ratio
Cocaine manufacture ̶ old conversion ratio
Cocaine seizures

36
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
Fig. 24
Growth in global opium production and global quantities of opiates seized, including
heroin, 1980–2018
Sources: UNODC, responses to the annual report questionnaire (for data on seizures); UNODC, opium poppy surveys, and
responses to the annual report questionnaire; and United States, Department of State, International Narcotics Control Strategy
Reports (for opium production estimates).
a
Applying a conversion ratio of 10 kg of opium per 1 kg of morphine or heroin.
0
50
100
150
200
250
300
350
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
Index: 1998 = 100
Opium production Heroin seizures Opiate seizures in heroin equivalents a
a

37
Alternative development
6
“international cooperation on eradicating the illicit
cultivation of crops used for the production of nar-
cotic drugs and psychotropic substances and on
alternative development” reflected the importance
of assessing the impacts of alternative development
not only on the basis of illicit crop estimates but
also on the basis of human development indicators.
The extent of the area under illicit crop cultivation
does not in itself reflect the sustainability of devel-
opment efforts and is not a sufficient indicator for
assessing the success of alternative development
interventions.
72
Experience has shown that short-
term reductions in illicit crop cultivation can be
quickly reversed, or cultivation can be displaced to
other locations, if interventions have not addressed
the root causes of illicit crop cultivation and pro-
vided sustainable solutions.
73
Evaluations of alternative development interventions
have largely relied on post-project implementation
reviews and not on rigorous impact assessments with
pre- and post-intervention analysis. Member States
have concurred that more efforts are required to
improve the impact assessments of alternative devel-
opment projects with a view to strengthen the
evidence base and further increase the effectiveness
of projects.
74
73 World Drug Report 2015. (United Nations publication, Sales
No. E.15.XI.6).
74 Outcome document of the thirtieth special session of the
General Assembly, entitled “Our joint commitment to effec-
tively addressing and countering the world drug problem”
(General Assembly resolution S-30/1, annex).
ALTERNATIVE
DEVELOPMENT
Alternative development is aimed at addressing
income- and non-income-related multidimensional
poverty and the lack of livelihood opportunities,
which are among the root causes of illicit drug crop
cultivation. The Political Declaration and Plan of
Action on International Cooperation towards an
Integrated and Balanced Strategy to Counter the
World Drug Problem of 2009, along with the
United Nations Guiding Principles on Alternative
Development of 2013, the outcome document of
the special session of the General Assembly, held in
2016, and the Ministerial Declaration on Strength-
ening Our Actions at the National, Regional and
International Levels to Accelerate the Implementa-
tion of Our Joint Commitments to Address and
Counter the World Drug Problem of 2019, have
placed alternative development high on the global
agenda as a development-oriented drug control
strategy.
72
Measuring the impact of alternative development
is challenging. Having recognized this fact, many
Member States sought to ensure that, in the 2009
Plan of Action, the recommendations relating to
72 UNODC. 2005. "Alternative Development: A Global
Thematic Evaluation. Final Synthesis Report".
Fig. 25
Theory of change in alternative development
Source: World Drug Report 2015 (United Nations publication, Sales No. E.15.XI.6).
Strengthening of
organized crime
and increasing
violence
Rising illicit
drug production
Reduction in
investment into
licit sectors
Reduction in
overall growth
of the licit
economy
Weakening of
the rule of law
Vicious
circle
Virtuous
circle
Alternative
development
Falling poverty
and strengthening
of the rule of law
Increase in
overall growth
of the licit
economy
Increase in
investment into
licit sectors
Weakening of
organized crime
and falling
violence
Falling illicit
drug production
38
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
An earlier analysis
75
by UNODC highlighted that
alternative development interventions, if well
designed, can help to address some of the underly-
ing factors and root causes of illicit crop cultivation
and can ultimately result in a sustainable reduction
in illicit crop cultivation in targeted regions through
integrated rural development. The analysis showed
that success in alternative development does not
come quickly, as it is dependent on long-term
investments that enhance human development,
gender equality and women’s empowerment, land
governance, security, the rule of law, institutional
presence and environmental management and
sustainability.
Other post-intervention analyses have been critical
of the effectiveness of alternative development
projects,
76
while others have been more optimistic
and have explained further the potential drivers of
75 Ibid.
76 Special Inspector General for Afghanistan Reconstruction,
Counternarcotics: Lessons from the U.S. Experience in Afghani-
stan (Arlington, Virginia, United States, 2018).
illicit crop cultivation and changes due to alterna-
tive development projects on the basis of theoretical
economic frameworks.
77
Understanding the drivers
of illicit crop cultivation remains at the core of the
design of evidence-based alternative development
projects and policies. These drivers continue to be
multifaceted and can differ depending on national
and local circumstances.
Factors influencing illicit crop
cultivation
Development gaps are the main factors
associated with illicit crop cultivation
Annual surveys of rural communities in Afghanistan
and Myanmar
78
have shown that villages affected
by illicit opium cultivation have a lower level of
77 Victoria A. Greenfield and others, Reducing the Cultivation
of Opium Poppies in Southern Afghanistan (Santa Monica,
California, RAND Corporation, 2015).
78 For example, UNODC annual socioeconomic reports on
Afghanistan and Myanmar.
Fig. 26
Development gap between villages affected and villages not affected by opium poppy cultivation
Source: UNODC and Afghanistan, Minister of Counter-Narcotics, Sustainable Development in an Opium Production Environment: Afghani-
stan Opium Survey Report 2016 (May 2017) and UNODC and Myanmar, Central Committee for Drug Abuse Control, Evidence for Enhanc-
ing Resilience to Opium Poppy Cultivation in Shan State, Myanmar. Implications for Alternative Development, Peace and Stability (March
2017).
Notes: The SDG indicators in the graphs are interpretative elements of the Sustainable Development Goal indicators, not the Sustainable Development
Goal indicators themselves, of which there are 247. The development gap refers to the difference in Sustainable Development Goal indicators between
villages affected (red line) and villages not affected (blue line) by illicit crop cultivation. The closer the lines are to the outside boundaries of the graphs,
the better the situation of the villages is in relation to the Sustainable Development Goal indicators.
Afghanistan Myanmar (Shan State)
0%
20%
40%
60%
80%
100%
SDG 1: No poverty
(Normalized income)
SDG 2: No hunger
(Coping without
reducing the number
of meals)
SDG 3: Health
(Availability of health
clinics)
SDG 4:
Education
(Availability
of schools)
SDG 5: Gender
equality (No
difference between
wages of men and
women)
SDG 6: Water and
sanitation (Availability
of good quality water)
SDG 7: Energy
(Availability of public
electricity)
SDG 8: Work
(Availability of internal
market to sell crops)
SDG 9: Infrastructure
(Availability of asphalt
roads)
SDG 10: Reduced
Inequalities (Income
allowing savings)
SDG 12: Responsible
consumption (No
collection of forest
wood for cooking)
SDG 13: Climate (No
crop shocks related to
climate change)
SDG 15: Life on land
(Non-deteriorated
quality of the forest)
SDG 16: Peace and
institutions
(Perception of safety)
Villages without poppy cultivation Villages with poppy cultivation
0%
20%
40%
60%
80%
100%
SDG 1: No poverty
(Normalized income)
SDG 2: No hunger
(Coping without
reducing the number
of meals)
SDG 3: Health
(Availability of health
clinics)
SDG 4:
Education
(Availability
of schools)
SDG 5: Gender
equality (No
difference between
wages of men and
women)
SDG 6: Water and
sanitation (Availability
of good quality water)
SDG 7: Energy
(Availability of public
electricity)
SDG 8: Work
(Availability of internal
market to sell crops)
SDG 9: Infrastructure
(Availability of asphalt
roads)
SDG 10: Reduced
Inequalities (Income
allowing savings)
SDG 12: Responsible
consumption (No
collection of forest
wood for cooking)
SDG 13: Climate (No
crop shocks related to
climate change)
SDG 15: Life on land
(Non-deteriorated
quality of the forest)
SDG 16: Peace and
institutions
(Perception of safety)
Villages without poppy cultivation Villages with poppy cultivation
0%
20%
40%
60%
80%
100%
Income
(SDG 1)
Food
security
(SDG 2)
Health care
(SDG 3)
Health care
for women
(SDG 3)
School
for boys
(SDG 4)
School
for girls
(SDG 4)
Electricity
(SDG 7)
Off-farm employment
(SDG 8)
Local market (SDG 8)
Roads
(SDG 9)
Public
transport
(SDG 9)
Farmers'
cooper at ives
(SDG 9)
Industries
(SDG 9)
Soil quality
(SDG 15)
Security
(SDG 16)
Government control
(SDG 16)
Villages without poppy cultivation
Villages with poppy cultivation

39
Alternative development
6
Fig. 27
Development gap between coca-growing
households and non-coca-growing households
in Colombia
Source: UNODC calculations using data from 6,000 households representing
the baseline for evaluation of the alternative development project entitled
“Land titling to substitute illicit crops” (“Formalizar para sustituir”) in 2017.
The baseline data reflect the situation before the beginning of the project.
Notes: The SDG indicators in the graphs are interpretative elements of the Sus-
tainable Development Goal indicators, not the Sustainable Development Goal
indicators themselves, of which there are 247. The development gap refers to the
difference in Sustainable Development Goal indicators between households culti-
vating illicit crops (red line) and households not cultivating illicit crops (blue line).
The closer the lines are to the outside boundaries of the graphs, the better the
situation of the households is in relation to the Sustainable Development Goal
indicators.
several of the multidimensional criteria for sustain-
able development (constituting what is referred to
here as a development gap) than villages not affected
by such cultivation. Analysed through the lens of
the Sustainable Development Goals, the comparison
of villages affected and not affected by illicit opium
cultivation suggests that different development fac-
tors drive farmers to engage in illicit cultivation. For
example, in 2017, in Afghanistan, the development
gap was particularly acute with regard to the Sus-
tainable Development Goals related to security and
access to health and education services, while in
Myanmar (Shan State) it was mostly associated with
the Sustainable Development Goals related to infra-
structure and natural resources.
79
In the same year,
in Colombia, a comparison among 6,000 house-
holds, located in 12 departments of the country,
showed that households cultivating coca had less
access to public services such as electricity and drink-
ing water than households not cultivating coca.
80
The development gap and inequality of opportuni-
ties differ not only between countries but also
between specific locations within a country; for
example, in 2017, in North Shan State in Myanmar,
they were largely related to water, sanitation and
energy, while in South Shan State, to deteriorating
natural resources.
81
Therefore, generalizations about
the drivers of illicit cultivation and the specific gaps
and inequalities of opportunities that alternative
development may be aimed at reducing could be
deceptive.
Drivers of illicit crop cultivation are
dynamic and cannot be explained by
income alone
Development gaps can result in unequal opportuni-
ties to access basic services required for individuals
79 UNODC and Afghanistan, Minister of Counter-Narcotics,
Sustainable Development in an Opium Production Environ-
ment: Afghanistan Opium Survey Report 2016 (May 2017);
and UNODC and Myanmar, Central Committee for Drug
Abuse Control, Evidence for Enhancing Resilience to Opium
Poppy Cultivation in Shan State, Myanmar: Implications for
Alternative Development, Peace and Stability (March 2017).
80 UNODC calculations using data from 6,000 households
representing the baseline for evaluation of the alternative
development project entitled “Land titling to substitute illicit
crops” (“Formalizar para sustituir”) in 2017. The baseline
data reflect the situation before the beginning of the project.
81 UNODC and Myanmar, Evidence for Enhancing Resilience to
Opium Poppy Cultivation in Shan State, Myanmar.
to sustain and improve their livelihoods, including
when the gaps relate to income disparities, and they
can drive different livelihood options (e.g., illicit
crop cultivation). However, illicit crop cultivation
is not always explained in terms of income differ-
ences. Sometimes there are no large differences, or
it is even the case that higher income is reported in
villages affected by illicit crop cultivation (although
overall income levels remain mostly low in both
types of communities), as profits derived from illicit
crops can be used to temporarily escape poverty
82
or to compensate for additional expenses associated
with the remoteness of the villages affected by illicit
crop cultivation. There are several factors that deter-
mine choices about cultivation, including security
82 Allan Gillies, John Collins and Alexander Soderholm,
“Addressing the development implications of illicit economies:
the rise of a policy and research agenda”, Journal of Illicit
Economies and Development, vol. 1, No. 1 (2019), pp.1–8.
0%
20%
40%
60%
80%
100%
SDG 1:
income > $1.9 per
person/day
SDG 3:
access to health
services
SDG 4:
secondary
school
SDG 5:
female as land
owner
SDG 6:
infrastructure
drinking water
SDG 7:
public electric
energy
SDG 9:
good quality
roads
SDG 12:
no cooking with
wood
SDG 13:
none affected by
climate change
Coca-growing households Non coca-growing households
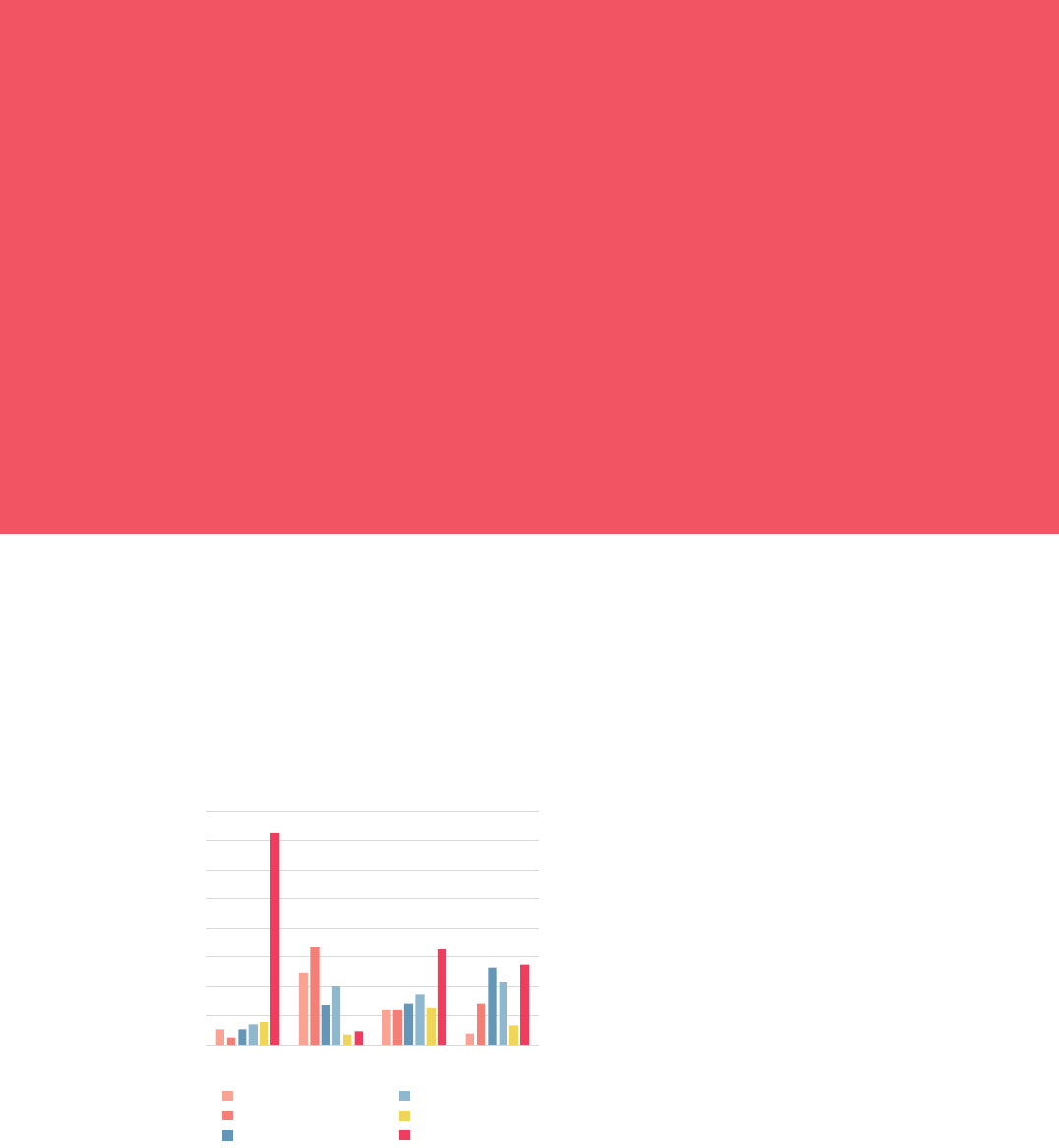
40
Female-headed households and illicit crop cultivation
Information about the participation of women in illicit
crop cultivation is scarce, and even more so on female-
headed households. A baseline survey in 2017 covering
16,100 households in 15 provinces in Afghanistan indi-
cated that female-headed households were less prone to
be involved in opium poppy cultivation than male-
headed households, as, in that country, the cultivation
of cash crops in general is typically a male activity,
whereas women are usually in charge of animal hus-
bandry and poultry.
Overall, female-headed households were in a critical
condition, characterized by lower annual earnings (up to
40 per cent less) than male-headed households. Female-
headed households were also found to have lower food
security, a lower degree of trust and confidence in
national authorities, and a higher number of household
members in search of employment. The survey findings
suggested that, in general, female-headed households
were more distressed by the conflict in Afghanistan than
male-headed households.
Source: UNODC, needs assessment and baseline report of the
Boost Alternative Development Interventions through Licit Liveli-
hoods and the Community-based Agriculture and Rural Develop-
ment East and West alternative development projects in
Afghanistan (2017).
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
due to greater living expenditure (for example, a
lack of schools or markets in the village, which
results in greater transport costs). However, a similar
or higher level of income does not always fully offset
the higher costs of living in those villages.
83
The drivers of illicit drug cultivation are dynamic
and can change a farmer’s attitude to illicit cultiva-
tion over time. For example, in Afghanistan it was
observed that, during a five-year period, some farm-
ers cultivated illicit crops every year, some did so
intermittently (from two to four times) and others
only once, while others were new to illicit cultivation
or had re-initiated it after a long-term break.
84
The
dynamic, versatile and context-specific nature of the
drivers of illicit cultivation prevent the development
of prescriptive solutions for successful alternative
development programmes. What is clear is that, for
an alternative development intervention to be effec-
tive, it must address the long-term root causes of the
development gap, which may be related to farmers’
livelihoods, households’ vulnerability to re-impov-
erishment, and to security and governance.
85
83 UNODC and Myanmar, Evidence for Enhancing Resilience to
Opium Poppy Cultivation in Shan State, Myanmar.
84 UNODC and Afghanistan, Sustainable Development in an
Opium Production Environment.
85 World Drug Report 2015; UNODC and Afghanistan, Sus-
tainable Development in an Opium Production Environment;
and UNODC and Myanmar, Evidence for Enhancing Resil-
ience to Opium Poppy Cultivation in Shan State, Myanmar.
and governance issues, but also deeper socioeco-
nomic disadvantages. In Myanmar, for example,
further analysis of the economic data indicates that
farmers in villages involved in illicit crop cultivation
earn slightly higher income but have significantly
smaller formal or informal savings than similar farm-
ers in villages not involved in illicit crop cultivation
Fig. 28
Reported frequency of opium poppy cultiva-
tion between 2012 and 2016 of farmers who
cultivated opium poppy in 2017, selected
regions, Afghanistan
Source: UNODC and Afghanistan, Minister of Counter-Narcotics,
Afghanistan Opium Survey 2017: Challenges to Sustainable Develop-
ment, Peace and Security (May 2018).
0
10
20
30
40
50
60
70
80
Eastern Northern Southern Western
Percentage of farmers who cultivated
opium poppy in 2017 and any time between
2012 and 2016
Newcomer 2017 1 of 5 years
2 of 5 years 3 of 5 years
4 of 5 years 5 of 5 years
0
10
20
30
40
50
60
70
80
Eastern Northern Southern Western
Percentage of farmers who cultivated
opium poppy in 2017 and any time between
2012 and 2016
Newcomer 2017 1 of 5 years
2 of 5 years 3 of 5 years
4 of 5 years 5 of 5 years
0
10
20
30
40
50
60
70
80
Eastern Northern Southern Western
Percentage of farmers who cultivated
opium poppy in 2017 and any time between
2012 and 2016
Newcomer 2017 1 of 5 years
2 of 5 years 3 of 5 years
4 of 5 years 5 of 5 years
0
10
20
30
40
50
60
70
80
Eastern Northern Southern Western
Percentage of farmers who cultivated
opium poppy in 2017 and any time between
2012 and 2016
Newcomer 2017 1 of 5 years
2 of 5 years 3 of 5 years
4 of 5 years 5 of 5 years
0
10
20
30
40
50
60
70
80
Eastern Northern Southern Western
Percentage of farmers who cultivated
opium poppy in 2017 and any time between
2012 and 2016
Newcomer 2017 1 of 5 years
2 of 5 years 3 of 5 years
4 of 5 years 5 of 5 years
0
10
20
30
40
50
60
70
80
Eastern Northern Southern Western
Percentage of farmers who cultivated
opium poppy in 2017 and any time between
2012 and 2016
Newcomer 2017 1 of 5 years
2 of 5 years 3 of 5 years
4 of 5 years 5 of 5 years
0
10
20
30
40
50
60
70
80
Eastern Northern Southern Western
Percentage of farmers who cultivated
opium poppy in 2017 and any time between
2012 and 2016
Newcomer 2017 1 of 5 years
2 of 5 years 3 of 5 years
4 of 5 years 5 of 5 years

41
Contribution of alternative development to female
income in Afghanistan
In Afghanistan, the Government, together with non-
governmental organizations, is currently implementing
with UNODC support a unique alternative develop-
ment project for the period 2017–2021 in 13 provinces
that focuses strongly on increasing female income. In
doing so, the project is contributing to peace and stabil-
ity, which are significantly associated with the reduction
of illicit crop cultivation. The project involves the ini-
tiation or strengthening of dairy and poultry produc-
tion, vegetable cultivation and orchard activities, with a
view to primarily enhancing female income, which usu-
ally only constitutes 5 to 10 per cent of total household
income.
The mid-term evaluation of the project, carried out in
2019, based on surveys of more than 4,000 households
in 220 villages, indicated that, in comparison with the
baseline in 2017, the number of households with female
members who generated income had increased from 21
to 29 per cent, as had income earned by women, by as
much as 10 per cent.
Source: UNODC, mid-term impact assessment of the Boost
Alternative Development Interventions through Licit Livelihoods
alternative development project in Afghanistan (2020).
Alternative development
6
Overview of alternative
development projects in the
period 2013–2017
In 2019, UNODC undertook a study to collect
information on the characteristics of alternative
development projects in terms of individual budg-
ets, main objectives, geographical coverage, duration
and implementing partners at the global level, with
the aim of understanding the scale of implementa-
tion of these projects.
The analysis represented one of the first efforts to
collect and systematize information on the status of
alternative development projects
86
worldwide. It
covered a total of 53 identified alternative develop-
ment projects that had been under implementation
during the period 2013–2017 in the countries where
most opium poppy is cultivated (Afghanistan,
Myanmar and Mexico
87
) and those where most coca
86 The analysis considers as an “alternative development” pro-
ject those aimed at improving the quality of life of farmers
and reduce or prevent the cultivation of illicit drug crops.
For simplification purposes, project also refers to pro-
gramme in the analysis.
87 In the case of Mexico, projects conducted in regions affected
by opium poppy cultivation did not explicitly include the
double objective of improving the quality of life of farm-
Fig. 29
Number of alternative development projects, by country and year, 2013–2017
Source: UNODC, “Research brief: global overview of alternative development projects, 2013–2017” (Vienna, 2019).
Note: N = 53. The numbers between brackets refer to the total number of projects under implementation each year.
0
2
4
6
8
10
12
14
16
2013 (N = 30) 2014 (N = 36) 2015 (N = 36) 2016 (N = 40) 2017 (N = 39)
Number
Afghanistan Colombia Peru Bolivia (Plurinational State of) Myanmar

42
is cultivated (Colombia, Peru and the Plurinational
State of Bolivia). These countries together accounted
for 98 per cent or more of the global cultivation of
opium poppy and coca in 2017,
88
the last year cov-
ered in the study.
89
Small increase in the total annual
budget of alternative development
projects worldwide driven by projects
in Colombia
The aggregated annual budget for all the alternative
development projects identified experienced a small
but gradual increase over the period 2013–2017,
from $190 million to $275 million. That was mainly
due to projects in Colombia, which more than dou-
bled their total annual budgets, from a combined
ers and reducing or preventing illicit crop cultivation. One
exception was the alternative development project “Rural
Development to discourage opium poppy cultivation in
Oaxaca, Guerrero and Michoacan”, conducted by the Food
and Agriculture Organization of the United Nations, but
it is not covered in this report, as it took place during the
period 1990–1993.
88 World Drug Report 2019 (United Nations publication, Sales
No. E.19.XI.9).
89 This analysis is based on an extensive review of data and
reports gathered from websites, supported by e-mail com-
munications and field visits to the offices of the main
international donors located in each of the six countries
mentioned.
total of $75 million in 2013 to $154 million in
2017. The growth was related to increased interest
in funding alternative development projects follow-
ing the peace agreement concluded with the
Revolutionary Armed Forces of Colombia (FARC)
in 2016, which included commitments towards the
voluntary cessation of illicit crop cultivation and the
implementation of social inclusion and development
projects. One of the largest alternative development
projects, the National Comprehensive Programme
for the Substitution of Illicit Crops (Plan Nacional
Integral de Sustitución de Cultivos de Uso Ilícito),
is funded by the Government of Colombia.
The total annual budget of projects in the Plurina-
tional State of Bolivia was also increased thanks to
funds provided by the European Union for two pro-
jects on integrated development with coca, one of
which started in 2014 and the other in 2016. In
Afghanistan and Myanmar, the total annual budget
for alternative development projects remained in
the same range over the period 2013–2017 (i.e.,
$77 million to $100 million in Afghanistan and
$3.4 million to $5.6 million in Myanmar). By con-
trast, funding for alternative development efforts in
Peru decreased from $34 million in 2013 to $26
million in 2017 as a result of a decrease in the
number of projects.
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
Fig. 30
Total annual budget of alternative development projects, by country, 2013–2017
Source: UNODC, “Research brief: global overview of alternative development projects, 2013–2017”.
Notes: N = 51. Two alternative development projects in Colombia were excluded as no official data on their budgets were publicly avail-
able. The total annual budget was estimated as the sum per year of the budgets of the alternative development projects after being
divided by the total duration of the projects in number of years. The numbers between brackets refer to the total number of projects
under implementation each year for which a budget was available.
0
20
40
60
80
100
120
140
160
180
200
220
240
260
280
2013
(N = 28)
2014
(N = 32)
2015
(N = 32)
2016
(N = 36)
2017
(N = 35)
Millions of dollars
Afghanistan
Colombia
Peru
Bolivia (Plurinational State of)
Myanmar

43
Most funding went to long-term
alternative development projects
Alternative development projects promote intricate
processes of behavioural change (e.g., farmers’ vol-
untary decisions to cease illicit crop cultivation) that
require long-term and continuous investment. A
budget analysis of the projects that ended between
2013 and 2017 showed that most of the funds were
spent on long-term projects. Out of a total budget
of $469 million allocated to completed projects over
the period 2013–2017, $382 million went to pro-
jects that lasted longer than six years, $81.3 million
to projects that lasted four to six years and $5.7
million to projects of less than four years.
Duration of the majority of completed
alternative development projects is too
short for sustainable results
While the largest share of the total combined budget
of the alternative development projects went to long-
term projects, in terms of the number of projects,
47 per cent of those completed lasted between four
and six years, and 12 per cent lasted less than four
years, which is likely to be too short for sustainable
results. The remaining 41 per cent of projects lasted
from 6 to 10 years. For both short- and long-term
alternative development projects, more efforts are
required to provide systematic and comparable evi-
dence of the sustainability of their effects on
reducing and preventing illicit crop cultivation and
community-based socioeconomic growth.
Fig. 32
Distribution of completed alternative
development projects, by individual
budget size and project duration,
2013–2017
Source: UNODC, “Research brief: global overview of alterna-
tive development projects, 2013–2017”.
Note: The data include 17 projects that were completed in 2017 or
before. The numbers between brackets refer to the total number
of completed projects for each category of project duration.
0
10
20
30
40
50
2 to <4 years
(N = 2)
4 to <6 years
(N = 8)
6 to 10 years
(N = 7)
Percentage
$100 million or more per project
$20 million to < $100 million per project
$5 million to < $20 million per project
$150,000 to < $5 million per project
Fig. 31
Total combined budget of completed
alternative development projects, by
duration of project, 2013–2017
Source: UNODC, “Research brief: global overview of alterna-
tive development projects, 2013–2017”.
Note: The data include 17 projects that were completed in 2017 or
before. The numbers between brackets refer to the total number
of completed projects for each category of project duration. No
project was completed during this period in the Plurinational State
of Bolivia.
0
25
50
75
100
125
150
175
200
225
250
275
300
325
350
375
400
2 to <4 years
(N = 2)
4 to <6 years
(N = 8)
6 to 10 years
(N = 7)
Millions of dollars
Afghanistan
Colombia
Peru
Myanmar
Alternative development
6

Impact assessments of alternative development interventions
in Afghanistan
UNODC, in cooperation with the Government, is cur-
rently evaluating the impacts of three large-scale alterna-
tive development projects in Afghanistan (with total
budgets of $20 million to $60 million each). The pro-
jects are being implemented by the Afghan Govern-
ment, two of them jointly with UNDP and one with
UNODC. The impact assessments are still ongoing and
include the monitoring of a comprehensive set of more
than 1,000 socioeconomic indicators and remote-sens-
ing analyses of land cover of more than 530 villages in
15 provinces (bi-)annually (from before the projects
began in 2017 until they end in 2022). To be able to
isolate the effects of the projects from external factors,
the impact assessments consider comparisons of both
socioeconomic indicators and land cover changes before
and after the implementation of the alternative develop-
ment projects between villages that receive the interven-
tions (referred to here as treatment villages) and similar
villages that do not receive them because they are located
outside the scope of the alternative development pro-
jects (referred to here as control villages). In this regard,
control villages are key for obtaining robust impact
evaluations.
For example, there was a significant reduction in opium
poppy areas (depicted in pink in the maps below) in
villages that received the alternative development inter-
ventions from 2017 to 2018. Nevertheless, a similar
reduction was also observed in control villages. If the
changes in opium poppy cultivation were purely due to
the alternative development projects, then the outcome
in the villages receiving the interventions would have
been different than in the control villages. The com-
parison between treatment and control villages helped
clarify that the changes in opium poppy cultivation in
2018 were mainly due to a drought, which affected both
types of village. The final results of the impact assess-
ments are expected to be available in 2022, once the
alternative development projects have ended.
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
44
Source: UNODC, needs assessment and baseline report of the Boost Alternative Development Interventions through Licit Livelihoods and
Community-based Agriculture and Rural Development East and West alternative development projects (2017); and UNODC, mid-term
impact assessments of the Community-based Agriculture and Rural Development East and West (2019).
Note: “Treatment villages” are those villages currently receiving the alternative development interventions. “Control villages” are similar villages that
are currently not receiving such interventions because they are outside the current scope of the alternative development projects.
Treatment village
2018
2017
Control village
20182017
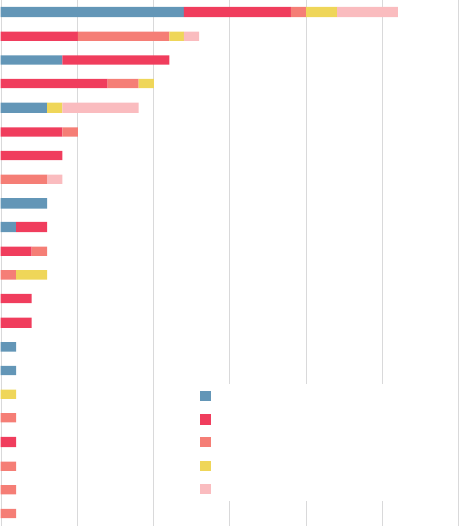
45
Alternative development
6
detailed information was available about the
amounts provided to individual implementing
partners.
Key objectives of alternative
development efforts vary greatly
between countries
The main stated purposes of the different alterna-
tive development projects, aside from reducing or
eliminating illicit crop cultivation, varied by country.
In Afghanistan, projects focused heavily on the
introduction of high-value crops (90 per cent of the
projects), in Myanmar, on food security (80 per
cent), in the Plurinational State of Bolivia, on the
social integration of native communities (70 per
cent), in Colombia, on supporting government
capacity, including territorial control (40 per cent),
and in Peru, on the consolidation of farmers’
Non-governmental organizations are
the main implementing partners in half
of all alternative development projects
Alternative development projects were usually
implemented by multiple partners, each responsible
for specific parts of the interventions, for example,
building infrastructure or providing training. Imple-
menting partners either conducted the interventions
themselves or hired or subcontracted other entities
and organizations. In half of the alternative devel-
opment projects, local non-governmental
organizations or private organizations participated
as implementing partners, mostly in projects with
budgets between $20 million and $100 million,
while UNODC was one of the implementing part-
ners in a quarter of the projects, mostly those with
individual budgets of less than $5 million. No
1
1
1
1
1
1
1
1
2
2
3
3
3
3
4
4
5
9
10
11
13
26
Access to internet and communication services
Assist counternarcotic policies and/or national agency
Change attitudes to increase farmer participation in projects
Land zonification and conservation areas
Public health
Reduce migration to coca departments
(Rural) employment, including off-farm activities
Reward counternarcotics achievements
Climate change (REDD+)
Land titling
Social integration (of native communities)
Support peace process and/or reduce violence
Competitiveness, incl. certifications
(Agri-)business services
Support previous eradication/avoid re-cultiv ation
Increase private sector investment
Education, incl. research
Food security
Counteract deforestation and/or natural resource conservation
Support to government capacity
Consolidate farmer associations and/or previous interventions
Introduction of high-value crops
0 5 10 15 20 25 30
Number of projects
Afghanistan
Colombia
Peru
Bolivia (Plurinational State of)
Myanmar
Fig. 33
Number of alternative development projects, by main objective and country, 2013–2017
Source: UNODC, “Research brief: global overview of alternative development projects, 2013–2017”.
Notes: N = 53. The main objectives are those as stated in the project documents and are not mutually exclusive. The numberes refer to the
number of projects for each stated main objective. The projects had one or more main objectives.

Estimates of the number of households cultivating illicit crops
worldwide
Reliable estimates of the total extent of illicit crop
areas are available from annual remote-sensing evalu-
ations carried out by UNODC together with the
countries where most opium poppy is cultivated
(Afghanistan, Mexico and Myanmar), and where
most coca is cultivated (Plurinational State of Bolivia,
Colombia and Peru). However, one of the most per-
sistent gaps in the decision-making process has been
the lack of systematic information about the global
number of households cultivating illicit crops.
Households may cultivate just one plot or several
small or large plots of illicit crops; some locations
with large total illicit crop areas may have a relatively
small number of such households, while others may
have a large number. Therefore, the total extent of
illicit crop areas does not alone provide an indication
of the number of households growing illicit crops.
On the basis of a methodology that combines data
from remote sensing, socioeconomic surveys and
agricultural censuses, the number of households cul-
tivating coca bush was estimated to range between
280,000 and 370,000, while those cultivating opium
poppy was estimated at between 325,000 and
600,000, resulting in an estimate of 605,000 to
970,000 households cultivating illicit crops in the six
countries most affected by coca bush and opium
poppy cultivation worldwide.
Any attempt to quantify the extent of the involve-
ment of households in illicit cultivation needs to
acknowledge the diversity of rural life. For example,
farmers may decide which legal crops to cultivate
based on the size and quality of their land, but they
may also base their decisions on external factors such
as crop prices at the local market. Many households
in rural areas also earn income from non-agricultural
activities such as wage labour on construction sites.
Such issues may explain fluctuations in household
income from year to year and affect wider household
decisions. As a result of these processes, data on the
number of households cultivating illicit crops can be
highly dynamic over time, especially in the case of an
annual crop such as opium poppy.
Number of households cultivating illicit crops
Source: UNODC, estimates made in 2019 of the number of households cultivating illicit crops worldwide.
Note: based on data on the Andean countries (Plurinational State of Bolivia, Colombia and Peru) and Mexico for 2017, and on Afghanistan
and Myanmar for 2018. The research on the number of households cultivating illicit crops was financially supported by Germany (Deutsche
Gesellschaft für Internationale Zusammenarbeit, GIZ).
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
1,000,000
Total households Households
cultivating opium
poppy
Households
cultivating coca
Number
Lower estimate Upper estimate
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
46
been covered by alternative development interven-
tions, even though investing there could potentially
pay off by preventing the expansion of illicit crop
cultivation. Ideally, such interventions, mostly
focused on prevention, would also include compre-
hensive impact assessments in order to provide strong
evidence of their effectiveness.
Difficult to assess the number of
households targeted by alternative
development projects
Reliable evidence on the number of households actu-
ally targeted by alternative development initiatives
remains scarce. Very few projects conducted baseline
and endline surveys or maintained reliable, continu-
ous tracking of project activities and results. By
contrast, information was generally provided about
the total number of households to be targeted by
the different projects, but aggregating that informa-
tion was complicated. Some projects were not clear
about the intended target group; in other cases, the
scope of the project was broad and also included
households that would indirectly benefit. Some of
the projects did not specify the number of target
households because they targeted aggregated units
such as schools, local community boards or coop-
eratives. Taking into account these limitations, the
best estimate for the number of households intended
to be targeted by alternative development interven-
tions in 2017 was 550,000. This estimate includes
households cultivating and households not cultivat-
ing illicit crops, as alternative development projects
are generally aimed at providing benefits to both
types of household to avoid the risk of creating “per
-
verse incentives” (i.e., an increase in illicit crop
cultivation by households not previously cultivating
illicit crops in an attempt to also benefit from alter-
native developments interventions).
associations, including the marketing of products
and extending previous interventions (40 per cent).
The introduction of high-value crops was one of
the most commonly stated main objectives of the
alternative development projects, with the exception
of those with small budgets of less than $150,000.
The main objectives of the large projects, with
budgets of more than $100 million, included
support to government capacity (for example, related
to the peace process in the case of Colombia) and,
to a minor extent, food security, improved
competitiveness of alternative development projects
(e.g., marketing assistance), increased farmer
participation in alternative development projects,
and off-farm activities. The smaller projects, with
budgets of less than $150,000, had as their main
objectives the counteracting of deforestation,
education and farmer association competitiveness.
Gradual shift away from focusing
mainly on high-value crops
Although the introduction of high-value crops was
one of the most common main objectives identified
in alternative development projects, despite differ-
ences among countries, the main focus of such
projects overall has shifted over time. While several
projects that started in the period 2013–2014
focused on the introduction of high-value crops, that
objective was slightly less common in the period
2016–2017. Moreover, some of the most recently
initiated alternative development projects are aimed
at addressing environmental issues, for example,
deforestation and forest degradation, in order to
access funding linked to climate change, land use
management and natural resource conservation, par-
ticularly in Colombia.
Areas with low but sharply increasing
levels of illicit crop cultivation are
being overlooked
Alternative development projects in Afghanistan and
Myanmar tended to be carried out in areas (provinces
or states) with traditionally high levels of illicit crop
cultivation. However, illicit crop cultivation has
recently started to emerge, in some cases at a steady
pace, in non-traditional locations such as Jowzjan
Province in Afghanistan and Chin State in Myanmar.
These emerging cultivation locations have not yet
Alternative development
6
47

48
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
other causalities and mere associations that may
characterize the intersection between drugs and vio-
lence, either indirectly or within a longer time frame,
as well as other research findings supporting the
existence of an inverse causality model whereby
engagement in criminal behaviour may also be a
factor leading to drug use.
92, 93
The psychopharmacological model refers to a poten-
tially increased propensity or vulnerability to
commit, or be the victim of, violence while under
the influence of psychoactive substances. This is
mainly understood to refer to substances that can
influence a person’s readiness to engage voluntarily
in criminal acts but may also include substances that
impair cognitive and psychomotor functions and
therefore increase the likelihood of unintentionally
committing crimes through negligence in potentially
fatal situations such as driving under the influence
of psychoactive substances. This model encompasses
violence perpetrated while the victim was under the
influence of a psychoactive substance such as sexual
assault or robbery because of the victim’s incapaci-
tation, as well as violence (e.g., physical attacks or
fights) committed while under the influence of
drugs.
94
Intimate partner violence, for example
against women, when the victim and/or the perpe-
trator is under the influence of psychoactive
substances, falls into this category.
The economic-compulsive model refers to people
– whether drug dependent or not – whose spending
on a psychoactive substance leads them to engage
in acquisitive or other income-generating crime in
order to fund their drug consumption. Such acquisi
-
tive crime (e.g., robbery, burglary or other forms of
theft) may or may not be violent. It can also involve
crimes such as selling drugs or sex work (where
criminalized).
The systemic model refers to violence that occurs
within illicit drug markets as part of the functioning
92 Serge Brochu, Drogue et criminalité: une relation complexe,
2nd ed. (Québec, Presses de l’Université de Montréal,
2006).
93 Helene Raskin White, “The drug use-delinquency con-
nection in adolescence”, in Drugs, Crime, and the Criminal
Justice System, Ralph A. Weisheit, ed., Academy of Criminal
Justice Sciences Monograph Series (Cincinnati, United
States, Anderson Publishers, 1990), pp. 215–256.
94 EMCDDA, Drugs and Crime: A Complex Relationship,
Drugs in Focus Series (Lisbon, 2007).
DRUGS AND VIOLENCE
The nexus between drugs and violence is a complex
issue with multiple facets. The purpose of this chap-
ter is to frame the issue rather than explore that
complexity in its entirety, and to offer some evidence
that illustrates key elements using the lens of the
tripartite framework developed by Paul Goldstein.
While he was the first scholar to conceptualize and
explain the relationship between drugs and
violence,
90
others since then have further elaborated
his framework and broadened it to apply it to the
analysis of a wider nexus: that between drugs and
crime.
91
The tripartite framework on
drugs and violence
The tripartite framework developed by Goldstein
considers drug use and drug trafficking as etiologi-
cal factors leading to violence and posits three causal
mechanisms or models, which are not mutually
exclusive, by which drugs can be directly linked to
violence in the short term: the psychopharmacologi-
cal, economic-compulsive and systemic models.
While the framework may apply differently depend-
ing on patterns of substance use, specific social
contexts, perpetrators’ motivations and victim ages
and types, the three models of drug-related violence
are assumed to transcend such differences, albeit
with nuances.
However, going beyond Goldstein’s tripartite frame-
work, it is important to acknowledge the myriad
90 Paul J. Goldstein, “The drugs/violence nexus: a tripartite
conceptual framework”, Journal of Drug Issues, vol. 15, No.
4 (1985), pp. 143–174.
91 See, for example, Philip Bean, Drugs and Crime (Devon,
United Kingdom, Willan Publishing, 2001); Trevor Ben-
nett and Katy Holloway, “Disaggregating the relationship
between drug misuse and crime”, Australian and New Zea-
land Journal of Criminology, vol. 38, No. 1 (April 2005),
pp. 102–121; Serge Brochu, Natalie Brunelle and Chantal
Plourde, Drugs and Crime: A Complex Relationship, 3rd ed.,
revised and expanded, Health and Society Series (Ottawa,
University of Ottawa Press, 2018); Robert MacCoun, Beau
Kilmer and Peter Reuter, “Research on drugs-crime linkages:
the next generation”, in Towards a Drugs and Crime Research
Agenda for the 21st Century, Special Report (Washington
D.C., United States Department of Justice, 2003); Helene
Raskin White and D. M. Gorman, “Dynamics of the drug-
crime relationship”, in The Nature of Crime: Continuity and
Change, vol. 1, Criminal Justice 2000 (Washington D.C.,
United States Department of Justice, 2000), pp. 151–218.
49
Drugs and violence
6
disputes.
100, 101
However, some have argued that the
greatest effect of drug use on violence may be indi-
rect, by creating a demand for the illicit production
and distribution of drugs.
102, 103
In addition, for a
variety of reasons, illegal markets can sometimes and
in some places generate enormous violence.
Economic compulsive and
psychopharmacological links
between psychoactive sub-
stances, violence and criminal
activity
Both the economic-compulsive and psychopharma-
cological models refer to the impact of drug use on
the behaviour of people who use drugs in terms of
their propensity to engage in violence or other crim-
inal activity.
Analysis of the limited data on homicides available
at the global level shows that the use of psychoactive
substances is associated with violent behaviour;
intoxication in particular is a significant factor in
homicide offences, although there is significant vari-
ability among countries. On the basis of data from
17 countries, it is estimated that 37 per cent of
homicide perpetrators were under the influence of
a psychoactive substance when committing the hom-
icide, and the vast majority tended to be under the
influence of alcohol.
104
This finding coincides with
100 Duane C. McBride and James A. Swartz, “Drugs and vio-
lence in the age of crack cocaine” in Drugs, Crime and the
Criminal Justice System, Ralph A. Weisheit, ed., Academy
of Criminal Justice Sciences Monograph Series (Cincinnati,
United States, Anderson Publishers, 1990), pp. 141–169.
101 Paul J. Goldstein and others, “Crack and homicide in New
York City, 1988: a conceptually-based event analysis”, Con-
temporary Drug Problems, vol. 16, No. 4 (January 1989), pp.
651–687.
102 Philip Keefer, Norman V. Loayza and Rodrigo R. Soares,
“The development impact of the illegality of drug trade”,
Policy Research Working Paper, No. 4543 (Washington
D.C., World Bank, 2008).
103 Drug demand, by creating the possibility of massive profits
for potential drug suppliers, may result in the emergence
of organized crime groups that make use of violence and
corruption as a means of survival and expansion. In some
countries, where drugs are produced, the proliferation of
organized crime groups may increase and lead to significant
levels of violence, to the extent that it poses a threat to
public safety.
104 UNODC, Global Study on Homicide 2019.
of such markets. It includes crime such as that which
occurs as a consequence of drug traffickers’ efforts
to maintain their illicit supply chains and maximize
profits. Systemic violence in this context is embedded
in the social and economic networks of drug market
actors, both drug traffickers at all levels of the supply
chain and drug users.
95
Manifestations of systemic
violence can be brutal and dramatic, since drug
traffickers and drug trafficking organizations may
resort to violence as a strategy of control to
intimidate competitors, enforce discipline among
their own ranks, assert control over territory and
trafficking routes and even challenge the State and
its law enforcement forces.
Multiple aspects of drug production, trafficking and
use, as well as law enforcement interventions imple-
mented by States in response to drug trafficking,
may contribute to different manifestations of crime
and violence.
96
People, including children, who use
drugs may be more susceptible to committing crime
than those who do not, in particular acquisitive and
other income-generating crime, which may or may
not have a violent character (for example, robbery
has a violent character, shoplifting does not). Drug
use is associated to a degree with homicidal violence,
but at a much lower rate than alcohol use.
97
How-
ever, there is also evidence of synergistic effects of
alcohol used in combination with drugs, cocaine in
particular as it can potentiate violent thoughts and
threats.
98
In addition, it has been shown, for exam-
ple, that during the “crack” cocaine epidemic which
started in the United States in 1984, the sharp
increase in the number of homicides
99
in many cities
could be attributed to the use of “crack” cocaine,
but also, and to a much greater degree, to systemic
violence, mostly resulting from territorial
95 Paul J. Goldstein, “The drugs/violence nexus”.
96 UNODC, Global Study on Homicide 2019 (Vienna, 2019).
97 Jeffrey Fagan, “Interactions among drugs, alcohol and vio-
lence”, Health Affairs, vol. 12, No. 4 (1993), pp. 65–79.
98 E. J. Pennings, A. P. Leccese and F. A. Wolff, “Effects of
concurrent use of alcohol and cocaine’, Addiction, vol. 97,
No. 7, (2002), pp. 773-783.
99 Alfred Blumstein, Frederick P. Rivara and Richard Rosen-
feld, “The rise and decline of homicide: and why”, Annual
Reviews of Public Health, vol. 21, 2000, pp. 505–541.

50
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
The association between domestic violence, includ-
ing male perpetrated intimate partner violence
against women, and psychoactive substance use has
been investigated extensively.
110
While it is not pos-
sible to ascertain a causal relationship between these
phenomena, evidence shows that women who were
injured by a male intimate partner are two to three
times more likely to abuse alcohol and to have used
cocaine than those who were not injured.
111, 112
While it is possible to argue that drug use can con-
tribute to crime, it is important to acknowledge that
the association between drug use and crime may
also be partly explained by mediating factors such
as poverty, unemployment, lack of education and
other forms of socioeconomic disadvantage as well
as other types of adversity, including those resulting
from individual factors, family circumstances and
peer influences. It is also important to acknowledge
in crime” (Washington D.C., Bureau of Justice Statistics,
United States Department of Justice, 1998).
110 Zilberman M.L. and Blume, S.B., “Domestic violence,
alcohol and substance use”, Brazilian Journal of Psychiatry,
vol. 27 (2005).
111 Miller, B.A. et. Al., ‘Family violence and victimization:
treatment issues for women with alcohol problems’,
Alcoholism: Clinical and Experimental Research, vol. 24,
No. 8 (2000).
112 Further information about drug use among women can be
found in booklet 5 of the present report.
a meta-analysis of 23 independent studies,
105
which
found that on average 37 per cent of homicide
offenders were under the influence of alcohol when
they committed the offence.
In the psychopharmacological model, the finding
that the role of alcohol in homicide is more impor-
tant than that of drugs
106
is mostly attributed to the
more widespread use of alcohol, which can also
occur in concomitance with the use of drugs.
107
The
existing body of research points to a positive but
not necessarily causal relationship between alcohol
use and violence.
108
Some studies analysing drug
consumption among inmates found that violent
offenders were more likely than non-violent offend-
ers to have consumed alcohol at the time of the
offence.
109
105 Joseph B. Kuhns and others, “The prevalence of alcohol-in-
volved homicide offending: a meta-analytic review”, Homi-
cide Studies, vol. 18, No. 3 (August 2014), pp. 251–270.
106 UNODC, Global Study on Homicide 2019.
107 William F. Wieczorek, John W. Welte and Ernest L. Abel,
“Alcohol, drugs and murder: a study of convicted homicide
offenders”, Journal of Criminal Justice, vol. 18, No. 3 (1990),
pp. 217–227.
108 Sara Markovitz, “Alcohol, drugs and violent crime”, Interna-
tional Review of Law and Economics, vol. 25, No. 1 (March
2005), pp. 20–44.
109 Lawrence A. Greenfield, “Alcohol and crime: an analysis
of national data on the prevalence of alcohol involvement
Fig. 34
Influence of psychoactive substances among perpetrators of homicides, latest available data,
2012–2015
Source: UNODC, homicide statistics.
Note: Based on data from 17 countries that provided sufficiently detailed breakdowns of perpetrators of homicides. For each country, only
the most recent data, up to 2015, were considered. The breakdown into cases of “under the influence” versus “no intoxication” has been
adjusted to take into account cases where the intoxication status was unknown. The breakdown into three kinds of intoxication adjusts for
cases in which multiple substance were involved.
Drugs
6%
Alcohol
90%
Other psychoac�ve
substances
4%
No
intoxica�on
63%
Under the
influence
37%

51
rigour in some contexts. While some studies attempt
to present causal associations between drug use and
criminal behaviour, often it is not possible to draw
any generalization from such findings, as they rely
on limited samples and do not always control for
other variables that may interfere with this associa-
tion, in particular when both may result from the
same risk factors or socioeconomic conditions. It
has been argued in particular that heroin use is more
strongly causally related to property crime than are
other drugs.
114
For example, injecting use of heroin
was associated with a 41 per cent increase in the
propensity to commit burglaries, robberies and
thefts in a longitudinal study of adolescents con-
ducted in the United States in the mid-1990s.
115
However, some of the better-documented patterns
of causations relate to cocaine and “crack” cocaine
use, especially in connection with acquisitive crime.
While studies in the 1980s have shown the associ-
ation between “crack” cocaine use and violent crime
in the United States, a more recent study on cocaine
114 United States, Office of National Control Drug Policy,
Improving the Measurement of Drug-related Crime (Washing-
ton D.C., October 2013).
115 Naci Mocan and Erdal Tekin, “Drugs and juvenile crime:
evidence from a panel of siblings and twin”, Advances in
Health Economics and Health Services Research, vol. 16, Sep-
tember 2005, pp. 91–120.
that drug use and criminal behaviour have many
risk factors in common, so the correlation between
drug use and crime may be spurious as it may stem
from risk factors associated with crime.
It is generally difficult to establish in a rigorous fash-
ion a causal relationship between the use of
psychoactive substances and criminal behaviour, as
being able to do so is highly dependent on the qual-
ity of the data and their coverage as well as the length
of the time frame used in the analysis. However,
such causality has been observed. One of the first
examples was a study conducted in the United States
in the early 1980s of a sample of men in Baltimore
suffering from heroin addiction, which found that
two thirds of them were regularly involved in crim-
inal behaviour and that the extent of their criminality
was influenced by their addiction status. Over the
11-year period analysed, findings showed that the
study participants committed more crime during
the periods when they were suffering from heroin
addiction than when they were not.
113
The role of drug use as a causal agent for criminal
behaviour has been investigated extensively in the
literature and is confirmed with a certain degree of
113 John C. Ball and others, “Lifetime criminality of heroin
addicts in the United States”, Journal of Drug Issues, vol. 12,
No. 3 (July 1982), pp. 225–239.
Challenges in measuring drug use-related criminality
There are a number of limitations in the measurement
and establishment of causality between drug use and
violence and with respect to the applicability of the
causal models developed by Goldstein.
Certain types of criminal acquisitive behaviour are vio-
lent (e.g., robbery), which makes it difficult to distin-
guish between the pharmacological and
economic-compulsive mechanisms when the perpetra-
tor is a person who uses drugs, or alcohol. In such cases,
the measurement of whether the perpetrator was under
the influence of psychoactive substances at the time of
the offence, which is seldom routinely measured, is
essential in order to qualify the relationship between
drug use and violence.
As far as the pharmacological model is concerned, the
use of dependence-inducing substances may also affect
a person’s inclination to violent behaviour because of
physical and emotional distress such as irritability, anxi-
ety and agitation, which are experienced during with-
drawal – when the person is not using any drug. This
may occur even when the substance that was used did
not have stimulant properties (e.g., heroin).
Furthermore, for both models, the simultaneous use of
multiple substances can also make it difficult to clearly
ascribe causality to a specific drug. This represents an
additional challenge in the case of the psychopharmaco-
logical model when the interaction between different
substances alters their pharmacological properties.
Drugs and violence
6
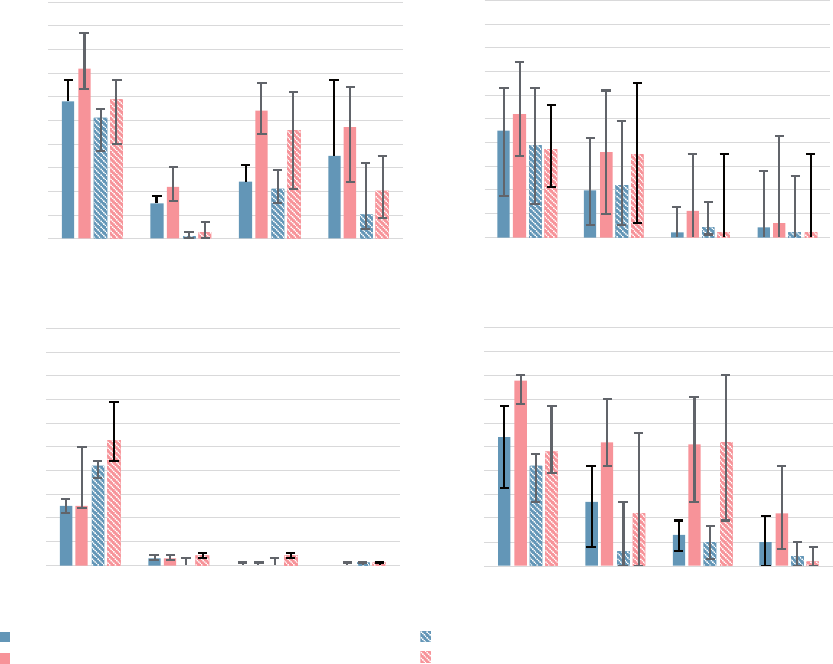
52
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
robberies and burglaries as a result of an increase in
– and in some cases a switch to – cocaine use in
people injecting drugs when heroin availability was
low. The increase in violent crime was attributed to
both the psychopharmacological effects of heavy
cocaine use and to a resulting increase in the finan-
cial need to fund that cocaine use.
Limited cross-national research available using data
collected throughout the calendar year 2000 on drug
use in arrestees from four countries (Australia,
use among people who were injecting drugs in Aus-
tralia during the “heroin drought” – a sudden
contraction of the heroin supply in Australia that
began in 2001 – showed evidence of a causal asso-
ciation between cocaine use and violent acquisitive
crime.
116
Both official crime data and interviews
with injecting drug users pointed to an increase in
116 Louisa Degenhardt and others, “Was an increase in cocaine
use among injecting drug users in New South Wales, Aus-
tralia, accompanied by an increase in violent crime?”, BMC
Public Health, vol. 5, No. 40 (April 2005), pp. 1–10.
Fig. 35
Drug use among male arrestees, by type of offence, Australia, South Africa, United Kingdom
and United States, 2000
Source: Bruce G. Taylor and others, “Monitoring the use of illicit drugs in four countries through the International Arrestee Drug
Abuse Monitoring (I-ADAM) program”, Criminal Justice, vol. 3, No. 3 (2003), pp. 269–286.
Note: The analysis is based on data from 4 cities in Australia, 3 in South Africa, 8 in the United Kingdom (England and Wales) and 28 in the
United States. Violent offences were defined as offences against the person. Drug use was self-reported and assessed through urine testing
within 48 hours of arrest.
0
10
20
30
40
50
60
70
80
90
100
Cannabis Cocaine Heroin Amphe-
tamines
Percentage
Australia
Annual prevalence of drug use: violent offences
Annual prevalence of drug use: property offences
Positive test results for drugs: violent offences
Positive test results for drugs: property offences
0
10
20
30
40
50
60
70
80
90
100
Cannabis Cocaine Heroin Amphe-
tamines
Percentage
United States
Annual prevalence of drug use: violent offences
Annual prevalence of drug use: property offences
Positive test results for drugs: violent offences
Positive test results for drugs: property offences
0
10
20
30
40
50
60
70
80
90
100
Cannabis Cocaine Heroin Amphe-
tamines
Percentage
South Africa
Annual prevalence of drug use: violent offences
Annual prevalence of drug use: property offences
Positive test results for drugs: violent offences
Positive test results for drugs: property offences
0
10
20
30
40
50
60
70
80
90
100
Cannabis Cocaine Heroin Amphe-
tamines
Percentage
United Kingdom (England and Wales)
Annual prevalence of drug use: violent offences
Annual prevalence of drug use: property offences
Positive test results for drugs: violent offences
Positive test results for drugs: property offences
0
10
20
30
40
50
60
70
80
90
100
Cannabis Cocaine Heroin Amphe-
tamines
Percentage
South Africa
Annual prevalence of drug use: violent offences
Annual prevalence of drug use: property offences
Positive test results for drugs: violent offences
Positive test results for drugs: property offences
0
10
20
30
40
50
60
70
80
90
100
Cannabis Cocaine Heroin Amphe-
tamines
Percentage
South Africa
Annual prevalence of drug use: violent offences
Annual prevalence of drug use: property offences
Positive test results for drugs: violent offences
Positive test results for drugs: property offences

53
Drugs and violence
6
England and Wales, South Africa and the United
States) has shown some association between drug
use and acquisitive crime; in particular, in certain
countries, a higher prevalence of drug use was
reported among arrestees for property offences than
among arrestees for violent offences,
117
with varia-
117 Bruce G. Taylor and others, “Monitoring the use of illicit
tions between countries in the use of different drugs
among arrestees and in the association with different
types of crime.
The systemic link: violence in
the context of drug trafficking
The association between drug trafficking and vio-
lence is not a linear one. Large-scale organized crime
activities, including international drug trafficking,
can take place without outbursts of violence when
stable criminal structures are in place, and/or cor-
ruption is endemic. For example, illegal drugs are
associated with very high violence levels in Colombia
and Mexico but not in Afghanistan, Bolivia (Pluri-
national State of), Peru and other drug-producing
and transit countries.
118
South-Eastern Europe also
offers a good example in this respect. Throughout
the 1990s, the simultaneous shocks of the Balkan
conflicts and the transition to a market economy
enabled organized crime actors in various countries
in the Balkan region to negotiate with State authori-
ties and entrench themselves in positions of relative
drugs in four countries through the International Arrestee
Drug Abuse Monitoring (I-ADAM) program”, Criminal
Justice, vol. 3, No. 3 (2003), pp. 269–286.
118 Francisco E. Thoumi, “Illegal drugs, anti-drug policy fail-
ure, and the need for institutional reforms in Colombia”,
Substance Use and Misuse, vol. 47, Nos. 8–9 (2012), pp.
972–1004.
Fig. 36
Drug use among male arrestees
a
in Chile, 1999
Source: International Arrestee Drug Abuse Monitoring Program I (I-ADAM), United States Department of Justice.
a
Based on a sample of 134 male arrestees from three detention centres in Santiago; includes arrestees detained for drug law offences.
b
Urine tests for tranquillizers refer specifically to benzodiazepines.
c
Urine tests from a subset of 90 arrestees.
0
10
20
30
40
50
60
70
Based on urine tests taken
upon arrest
c
Self-reported use - at least once in
the previous 3 months
Percentage of arrestees tes�ng
posi�ve / self-repor�ng use of substanc
e
Cannabis
Cocaine
Alcohol
Tranquillizers
b
Amphetamines
Fig. 37
Homicide rates in South-Eastern
Europe, selected countries, 2000–2016
Source: UNODC, homicide statistics.
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
Rate per 100,000 population
Serbia
Bosnia and Herzegovina
Romania
Bulgaria
Croatia
North Macedonia

54
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
attributed to slow-moving social indicators such as
income inequality; organized crime offers a more
plausible explanation.
126
Some research has shown that law enforcement and
policing targeting the upper echelons of drug traf-
ficking chains that generate the highest profits and
most violence are more effective at reducing violence
than is indiscriminate law enforcement by authori-
ties.
127
For example, police interventions that target
the most violent drug traffickers can reduce violence
by creating a powerful deterrent to violent behav-
ior.
128
A systematic review of 15 studies on the
impact of drug law enforcement on drug market
violence has shown that an increase in drug law
enforcement involving targeted crackdowns by mili-
tary or police forces is unlikely to reduce drug
market violence. While disrupting drug markets and
in particular organized crime groups involved in
drug distribution, this type of law enforcement
intervention has been found, paradoxically, to lead
to an increase in gun violence and in the homicide
rate as new protagonists seize opportunities to enter
126 UNODC, Global Study on Homicide 2019.
127 World Drug Report 2016 (United Nations publication, Sales
No. E.16.XI.7), p. 98.
128 Mark Kleiman, “Surgical strikes in the drug wars: smarter
policies for both sides of the border”, Foreign Affairs, vol.
90, No. 5 (September/October 2011), pp. 89–101.
impunity.
119
Following a spike after the fall of the
Berlin Wall, homicide rates in most South-Eastern
European countries have been low and declining,
although large quantities of heroin have continued
to transit the region. It has been estimated that
between 2009 and 2012, opiates trafficked along
the Balkan route generated an average gross profit
of $28 billion per year.
120
The presence and level of violence is dependent not
so much on the quantities trafficked as on certain
changes that produce instability in the balance of
power between organized crime groups. Several fac
-
tors can cause such instability, including changes in
the size of illicit markets,
121
the death or incarcera-
tion of high-profile leaders
122
and law enforcement
measures that weaken one group relative to anoth-
er.
123
Furthermore, interventions by law enforcement
can disrupt the apparent steadiness brought about
by illicit trafficking and lead to instability and out-
bursts of violence in society. Events in Mexico and
in the countries of the Northern Triangle of Central
America (El Salvador, Guatemala and Honduras)
between 2007 and 2011 offer a striking example of
how the destabilization caused by shifts in illegal
drug markets affected the level of violence.
124
Within
that period of time, the homicide rate
125
increased
threefold in Mexico: such a rapid shift cannot be
119 UNODC, Crime and its Impact on the Balkans and Affected
Countries (March 2008).
120 UNODC, Drug Money: The Illicit Proceeds of Opiates Traf-
ficked on the Balkan Route (2015).
121 For example, in Honduras between 2007 and 2011. See
UNODC, Global Study on Homicide 2019.
122 Gabriela Calderon and others, “The beheading of criminal
organizations and the dynamics of violence in Mexico”,
Journal of Conflict Resolution, vol. 59, No. 8 (June 2015).
123 In 2008, it was alleged that Mexican enforcement action
improved the situation of the Sinaloa Federation relative to
their rivals, emboldening them to increase violent reprisals.
See Ioan Grillo, El Narco: Inside Mexico’s Criminal Insurgency
(New York, Bloomsbury Press, 2011), pp. 117–118.
124 For an analysis of the trafficking flows in Mexico and the
Northern Triangle, the turf war between drug cartels and the
fluctuation of homicide rates, see UNODC, Global Study on
Homicide 2019.
125 Violence is a much broader concept than homicide and can
manifest itself in different ways. Homicide, the intentional
killing of another person, is the most severe manifestation
of violence. Situations in which organized criminal groups
are in control of a territory may lead to a decrease in levels
of lethal violence and an increase in other forms of violence,
such as extortion, intimidation, and human rights viola-
tions.
Fig. 38
Homicide rates in Honduras and Mexico,
2007–2018
Source: UNODC, homicide statistics, and national sources.
0
5
10
15
20
25
30
35
0
10
20
30
40
50
60
70
80
90
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
Homicide rate in Mexico
(victims per 100,000 population)
Homicide rate in Honduras
(victims per 100,000 population)
Honduras
Mexico
55
Drugs and violence
6
the market and competition increases.
129
As illustrated by the example of South-Eastern
Europe, drug trafficking can occur without violence.
The so-called “pax mafiosa”, a set of alliances made
between national organized crime groups in Europe
observed in the 1990s, after the fall of the commu-
nist regimes, signalled the emergence of cooperation
between various organized crime groups.
130
Those
groups sought to work together, transcending
national borders and dividing the proceeds from
transnational illicit businesses between themselves.
The main idea behind that shift in strategies and
operations was that cooperation served their interest
better than did conflict. However, the situation of
organized crime groups in Southern Europe has
evolved since the 1990s. In Montenegro, the his-
torical conflict between criminal groups has spilled
over into Serbia and Bosnia and Herzegovina as a
result of long-standing feuds between powerful
groups in the criminal underworld of Montenegro
and Serbia.
131
129 Dan Werb and others, “Effect of drug law enforcement on
drug market violence: a systematic review”, International
Journal of Drug Policy, vol. 22, No. 2 (March 2011), pp.
82–94.
130 Claire Sterling, Crime without frontiers: The Worldwide
Expansion of Organised Crime and the Pax Mafiosa, (London,
Little Brown, 1994).
131 Global Initiative against Transnational Organised Crime,
“Hotspots of organised crime in the Western Balkans: local
vulnerabilities in a regional context” (Geneva, 2019).

56
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
DRUGS AND THE CRIMINAL
JUSTICE SYSTEM
In 2018, an estimated 10.7 million people world-
wide were held in prisons, either in pre-trial
detention or because they had been convicted of
criminal offences.
132
In 2017 (the latest year for
which data were available), an estimated 714,000
women,
133
or around 7 per cent of the prison popu-
lation, were held in prisons.
Cannabis is the drug that brings
most people into contact with
the criminal justice system at
the global level
While data on people suspected of drug law offences
should be interpreted with caution as they reflect a
multitude of factors such as national drug policies,
priorities and targeting strategies, as well as the activ-
ities and effectiveness of drug law enforcement in
different countries, on the basis of reports from a
total of 69 countries over the period 2014–2018,
overall many more men than women were brought
132 Roy Walmsley, “World prison population list”, 12th ed.
(London, Institute for Criminal Policy Research, 2018).
133 Roy Walmsley, “World female imprisonment list”, 4th ed.
(London, Institute for Criminal Policy Research, 2017).
into contact with the criminal justice system for
either drug possession for personal use or drug traf-
ficking (88 per cent were men). Among the four
main drug types – ATS, cannabis, cocaine and opi-
oids – for which data were reported, cannabis
accounted for more than half of those brought into
contact with the criminal justice system over the
five-year period (reflecting the large global market
for the drug), followed by ATS (19 per cent), cocaine
(11 per cent) and opioids (7 per cent).
However, the situation in some regions diverges sig-
nificantly from the overall global picture, because
of either national policies, law enforcement strate-
gies and practices, or the different vulnerabilities of
users and traffickers of different substances to law
enforcement activities.
Data show that, after cannabis, the drug for which
the most people are brought into contact with the
criminal justice system is the drug that dominates
the market in a particular region. In Asia in particu-
lar, ATS are the major drug group for which people
are brought into contact with the criminal justice
system, most likely as a result of the wide use and
trafficking of methamphetamine in the region. For
Fig. 39
Estimated number of people in the criminal justice system for drug offences
Source: United Nations Survey of Crime Trends and Operations of Criminal Justice Systems (various years, latest data available).
1,900,000
860,000
470,000
1,200,000
740,000
1,700,000
3.1 million arrested 1.6 million convicted 2.2 million in prison:
sentenced
drug possession for personal use
drug trafficking
Trafficking 39%
Use 61%
Trafficking 56%
Use 54%
Trafficking 78%
Use 22%

57
Drugs and the criminal justice system
6
Fig. 40
Distribution of men and women brought into contact with the criminal justice system for
drug law offences, by drug type and region, 2014–2018
Source: UNODC, responses to the annual report questionnaire.
Note: The data presented in this graph are based on the percentage of men and women brought into contact with the criminal justice
system by drug type, for possession for personal use or trafficking over the period 2014–2018. During that period, a total of 69 countries
– 14 in Africa, 18 in the Americas, 14 in Asia, 21 in Europe and 2 in Oceania (Australia and New Zealand) – reported data on the number
of people brought into contact with the criminal justice system. In Africa and Asia, more countries reported on the number of people
brought into contact with the criminal justice system for possession of drugs than for drug trafficking. In the remaining regions, the same
number of countries reported for either type of offence. The data were not weighted by the population of the region.
0
10
20
30
40
50
60
70
80
90
100
Drug trafficking: men
Drug trafficking: women
Drug possession/use: men
Drug possession/use: women
Drug trafficking: men
Drug trafficking: women
Drug possession/use: men
Drug possession/use: women
Drug trafficking: men
Drug trafficking: women
Drug possession/use: men
Drug possession/use: women
Drug trafficking: men
Drug trafficking: women
Drug possession/use: men
Drug possession/use: women
Drug trafficking: men
Drug trafficking: women
Drug possession/use: men
Drug possession/use: women
Africa Americas Asia Europe Oceania
Percentage
Amphetamine-type stimulants Cannabis Cocaine Opioids
Women who are incarcerated
for drug-related offences suffer
long-lasting consequences
Women often suffer serious long-term consequences
of incarceration that affect several aspects of their
lives. In most instances, on the basis of gender-neu-
tral policies and practices, women are subject to the
same correctional procedures as are men, despite
the fact that correctional services and procedures
are designed for men.
134
Both drug use and incar-
ceration carry stigma for both men and women, but
the degree of stigma is much greater for women and
may be additive, because of gender-based stereotypes
that hold women to different standards.
135
For
134 Stephanie S. Covington and Barbara E. Bloom, “Gendered
justice: women in the criminal justice system”, in Gendered
Justice: Addressing Female Offenders, Barbara E. Bloom, ed.
(Durham, North Carolina, Carolina Academic Press, 2003).
135 Juliana van Olphen and others, “Nowhere to go: how stigma
both males and females, offences related to ATS are
predominant among those brought into contact
with the criminal justice system for possession for
personal use. In the case of trafficking, the data show
different patterns for men and women. Among those
brought into contact with the criminal justice system
for drug trafficking in Asia, for those who are men,
ATS, opioids and cannabis account for similar pro-
portions of cases (each drug group accounts for
about a third of cases), while for women, ATS
account for 60 per cent of cases, followed by opioids
(which account for a third).
Cocaine-related offences are particularly prevalent
in the Americas, reflecting the extent of cocaine
supply and trafficking in the region. Among those
brought into contact with the criminal justice system
for drug trafficking in the Americas, cocaine
accounts for about 40 per cent, with similar propor-
tions of men and women.
58
WORLD DRUG REPORT 2020
OTHER DRUG POLICY ISSUES
example, women using drugs or being involved in
criminal activity are seen as contravening the tradi-
tional role of mothers and care givers.
136
Therefore
a formerly incarcerated woman may be treated
poorly by others, denied access to housing or
employment because of her criminal history, or
internalize feelings of worthlessness because of the
lowered expectations of those around her.
Women in prison may also have a long history of
abuse and mental health issues. For example, women
charged with drug-related offences often suffer from
substance use disorders, psychiatric disorders and a
history of physical and sexual abuse.
137
Also, research
shows that many women arrested for drug-related
offences, in particular drug trafficking, have been
victims of trafficking in persons or sex trafficking
and forced to carry drugs.
138, 139
However, while in
prison, few women are provided with the health-
care services necessary to address their drug use
disorders, other co-morbidities or reproductive
health issues. In addition, women prisoners may
suffer particular emotional and mental health con-
sequences resulting from the disruption of family
ties, as they are more likely to be incarcerated a
greater distance from home than are men, which
has a particularly harmful impact on mothers and
their prospects of resettlement.
140, 141, 142, 143, 144
limits the options of female drug users after release from
jail”, Substance Abuse Treatment, Prevention, and Policy, vol.
4, No. 10 (May 2009).
136 UNODC, World Drug Report 2018, Booklet 5: Women
(United Nations publication, Sales No Sales No. E.18.XI.9).
137 Ernest Drucker, “Drug law, mass incarceration, and public
health”, Oregon Law Review, vol. 91, No. 4 (2013), pp.
1097–1128.
138 Louise Shelley, “The relationship of drug and human traf-
ficking: a global perspective”, European Journal on Criminal
Policy and Research, vol. 18, No. 3 (September 2012). The
author argues that drug trafficking is linked to several forms
of trafficking, such as labour trafficking in the agricultural
sector and sex trafficking. Some smuggled individuals often
pay for their movement to their destination by being drug
couriers. In addition, drugs may be used to recruit new
victims.
139 UNODC and Colombia, Ministry of Justice and Law,
Caracterización de Condiciones Socioeconómicas de Mujeres
relacionadas con Problemas de Drogas: Las Mujeres Privadas
de la Libertad por Delitos de Drogas (Bogotá, 2019).
140 Penal Reform International, Who Are Women Prisoners?
Survey Results from Armenia and Georgia (London, 2013).
141 Penal Reform International, Who Are Women Prisoners?
Survey Results from Armenia and Georgia (London, 2013).
Moreover, incarcerated women do not generally
receive sufficient support to prepare for their return
to their families, intimate partners and the
community. Not only do women have fewer
opportunities to access education, work and training
programmes in prison than do men, but also the
skills they learn in prison are mainly recreational
and are based on gender stereotypes and thus often
fail to provide women with financial remuneration
and do not necessarily provide them with skills that
are suitable for the current job market upon their
release.
145, 146
Upon release, women face stigma in
the community because of their drug use and
incarceration, resulting in an even greater challenge
for them to access the health-care and social services
that they need, such as housing and employment
services. They may therefore end up in a situation
of social isolation and social exclusion, leaving them
to continue living in circumstances of social and
economic disadvantage and inequality. In particular,
incarcerated women re-entering the community also
need to navigate between both the relationships that
put them at risk for either drug use or criminality
and the relationships that they will rely on for
support after their release. This is complicated by
the fact that the only relationships that they may
have could have been those contributing, in the first
place, to their problems, including drug use, mental
health issues or criminality.
147
142 Penal Reform International, Who Are Women Prisoners?
Survey Results from Kazakhstan and Kyrgyzstan (London,
2014).
143 Penal Reform International, Who Are Women Prisoners?
Survey Results from Jordan and Tunisia (London, 2014).
144 Penal Reform International, Who Are Women Prisoners?
Survey Results from Uganda (London, 2015).
145 Marta Cruells, Noelia Igareda and SURT Association, eds.,
Women, Integration and Prison (Barcelona, Aurea Editores,
2005).
146 Ana T. Cárdenas, Mujeres y Cárcel: Diagnóstico de las Necesi-
dades de Grupos Vulnerables en Prisión (Santiago de Chile,
Universidad Diego Portales-ICSO, 2010).
147 Claire Snell Rood and others, “Incarcerated women's rela-
tionship-based strategies to avoid drug use after community
re-entry”, Women Health, vol 56. No 7 (October 2016), pp
843-858.

59
GLOSSARY
amphetamine-type stimulants — a group of sub-
stances composed of synthetic stimulants controlled
under the Convention on Psychotropic Substances
of 1971 and from the group of substances called
amphetamines, which includes amphetamine, meth-
amphetamine, methcathinone and the
“ecstasy”-group substances (3,4-methylenedioxym-
ethamphetamine (MDMA) and its analogues).
amphetamines — a group of amphetamine-type
stimulants that includes amphetamine and
methamphetamine.
annual prevalence — the total number of people of
a given age range who have used a given drug at
least once in the past year, divided by the number
of people of the given age range, and expressed as a
percentage.
coca paste (or coca base) — an extract of the leaves
of the coca bush. Purification of coca paste yields
cocaine (base and hydrochloride).
“crack” cocaine — cocaine base obtained from
cocaine hydrochloride through conversion processes
to make it suitable for smoking.
cocaine salt — cocaine hydrochloride.
drug use — use of controlled psychoactive substances
for non-medical and non-scientific purposes, unless
otherwise specified.
fentanyls - fentanyl and its analogues.
new psychoactive substances — substances of abuse,
either in a pure form or a preparation, that are not
controlled under the Single Convention on Narcotic
Drugs of 1961 or the 1971 Convention, but that
may pose a public health threat. In this context, the
term “new” does not necessarily refer to new inven-
tions but to substances that have recently become
available.
opiates — a subset of opioids comprising the various
products derived from the opium poppy plant,
including opium, morphine and heroin.
opioids — a generic term that refers both to opiates
and their synthetic analogues (mainly prescription
or pharmaceutical opioids) and compounds synthe-
sized in the body.
problem drug users — people who engage in the
high-risk consumption of drugs. For example,
people who inject drugs, people who use drugs on
a daily basis and/or people diagnosed with drug use
disorders (harmful use or drug dependence), based
on clinical criteria as contained in the Diagnostic
and Statistical Manual of Mental Disorders (fifth edi-
tion) of the American Psychiatric Association, or
the International Classification of Diseases and Related
Health Problems (tenth revision) of WHO.
people who suffer from drug use disorders/people with
drug use disorders — a subset of people who use
drugs. Harmful use of substances and dependence
are features of drug use disorders. People with drug
use disorders need treatment, health and social care
and rehabilitation.
harmful use of substances — defined in the Interna-
tional Statistical Classification of Diseases and Related
Health Problems (tenth revision) as a pattern of use
that causes damage to physical or mental health.
dependence — defined in the International Statistical
Classification of Diseases and Related Health Problems
(tenth revision) as a cluster of physiological, behav-
ioural and cognitive phenomena that develop after
repeated substance use and that typically include a
strong desire to take the drug, difficulties in control-
ling its use, persisting in its use despite harmful
consequences, a higher priority given to drug use
than to other activities and obligations, increased
tolerance, and sometimes a physical withdrawal
state.
substance or drug use disorders — referred to in the
Diagnostic and Statistical Manual of Mental Disorders
(fifth edition) as patterns of symptoms resulting
from the repeated use of a substance despite expe-
riencing problems or impairment in daily life as a
result of using substances. Depending on the
number of symptoms identified, substance use dis-
order may be mild, moderate or severe.
prevention of drug use and treatment of drug use dis-
orders — the aim of “prevention of drug use” is to
prevent or delay the initiation of drug use, as well
as the transition to drug use disorders. Once a person
develops a drug use disorder, treatment, care and
rehabilitation are needed.

61
REGIONAL GROUPINGS
The World Drug Report uses a number of regional
and subregional designations. These are not official
designations, and are defined as follows:
•
East Africa: Burundi, Comoros, Djibouti, Eritrea,
Ethiopia, Kenya, Madagascar, Mauritius, Rwanda,
Seychelles, Somalia, South Sudan, Uganda,
United Republic of Tanzania and Mayotte
•
North Africa: Algeria, Egypt, Libya, Morocco,
Sudan and Tunisia
•
Southern Africa: Angola, Botswana, Eswatini,
Lesotho, Malawi, Mozambique, Namibia, South
Africa, Zambia, Zimbabwe and Reunion
•
West and Central Africa: Benin, Burkina
Faso, Cabo Verde, Cameroon, Central African
Republic, Chad, Congo, Côte d’Ivoire,
Democratic Republic of the Congo, Equatorial
Guinea, Gabon, Gambia, Ghana, Guinea,
Guinea-Bissau, Liberia, Mali, Mauritania, Niger,
Nigeria, Sao Tome and Principe, Senegal, Sierra
Leone, Togo and Saint Helena
•
Caribbean: Antigua and Barbuda, Bahamas,
Barbados, Cuba, Dominica, Dominican Republic,
Grenada, Haiti, Jamaica, Saint Kitts and Nevis,
Saint Lucia, Saint Vincent and the Grenadines,
Trinidad and Tobago, Anguilla, Aruba, Bonaire,
Netherlands, British Virgin Islands, Cayman
Islands, Curaçao, Guadeloupe, Martinique,
Montserrat, Puerto Rico, Saba, Netherlands, Sint
Eustatius, Netherlands, Sint Maarten, Turks and
Caicos Islands and United States Virgin Islands
•
Central America: Belize, Costa Rica, El Salvador,
Guatemala, Honduras, Nicaragua and Panama
•
North America: Canada, Mexico and United
States of America, Bermuda, Greenland and Saint-
Pierre and Miquelon
•
South America: Argentina, Bolivia (Plurinational
State of), Brazil, Chile, Colombia, Ecuador,
Guyana, Paraguay, Peru, Suriname, Uruguay,
Venezuela (Bolivarian Republic of), Falkland
Islands (Malvinas) and French Guiana
•
Central Asia and Transcaucasia: Armenia,
Azerbaijan, Georgia, Kazakhstan, Kyrgyzstan,
Tajikistan, Turkmenistan and Uzbekistan
•
East and South-East Asia: Brunei Darussalam,
Cambodia, China, Democratic People’s Republic
of Korea, Indonesia, Japan, Lao People’s
Democratic Republic, Malaysia, Mongolia,
Myanmar, Philippines, Republic of Korea,
Singapore, ailand, Timor-Leste, Viet Nam,
Hong Kong, China, Macao, China, and Taiwan
Province of China
•
South-West Asia: Afghanistan, Iran (Islamic
Republic of) and Pakistan
•
Near and Middle East: Bahrain, Iraq, Israel,
Jordan, Kuwait, Lebanon, Oman, Qatar, Saudi
Arabia, State of Palestine, Syrian Arab Republic,
United Arab Emirates and Yemen
•
South Asia: Bangladesh, Bhutan, India, Maldives,
Nepal and Sri Lanka
•
Eastern Europe: Belarus, Republic of Moldova,
Russian Federation and Ukraine
•
South-Eastern Europe: Albania, Bosnia and
Herzegovina, Bulgaria, Croatia, Montenegro,
North Macedonia, Romania, Serbia, Turkey and
Kosovo
148
•
Western and Central Europe: Andorra, Austria,
Belgium, Cyprus, Czechia, Denmark, Estonia,
Finland, France, Germany, Greece, Hungary,
Iceland, Ireland, Italy, Latvia, Liechtenstein,
Lithuania, Luxembourg, Malta, Monaco,
Netherlands, Norway, Poland, Portugal, San
Marino, Slovakia, Slovenia, Spain, Sweden,
Switzerland, United Kingdom of Great Britain
and Northern Ireland, Faroe Islands, Gibraltar
and Holy See
Oceania (comprised of four sub-regions):
•
Australia and New Zealand: Australia and New
Zealand
•
Polynesia: Cook Islands, Niue, Samoa, Tonga,
Tuvalu, French Polynesia, Tokelau and Wallis and
Futuna Islands
•
Melanesia: Fiji, Papua New Guinea, Solomon
Islands, Vanuatu and New Caledonia
•
Micronesia: Kiribati, Marshall Islands, Micronesia
(Federated States of), Nauru, Palau, Guam and
Northern Mariana Islands
148 All references to Kosovo in the World Drug Report should
be understood to be in compliance with Security Council
resolution 1244 (1999).

Presented in six separate booklets, the World Drug Report 2020 provides a wealth of
information and analysis to support the international community in implementing
operational recommendations on a number of commitments made by Member
States, including the recommendations contained in the outcome document of the
special session of the General Assembly on the world drug problem, held in 2016.
Booklet 1 provides a summary of the five subsequent booklets by reviewing their
key findings and highlighting their policy implications. Booklet 2 focuses on drug
demand and contains a global overview of the extent of and trends in drug use,
including drug use disorders, and its health consequences. Booklet 3 deals with drug
supply and presents the latest estimates and trends regarding the production of and
trafficking in opiates, cocaine, amphetamine-type stimulants and cannabis. Booklet
4 addresses a number of cross-cutting issues, including the macrodynamics that are
driving the expansion and increasing complexity of the drug markets, and describes
some of the rapidly evolving drug-related concerns: the latest, multifaceted global
opioid crisis; rapid market changes; the market for new psychoactive substances;
the use of the darknet for supplying drugs; and developments in jurisdictions that
have measures allowing the non-medical use of cannabis. Booklet 5 looks at the
association between socioeconomic characteristics and drug use disorders, including
at the macro-, community and individual levels, with a special focus on population
subgroups that may be impacted differently by drug use and drug use disorders.
Finally, booklet 6 addresses a number of other drug policy issues that all form part
of the international debate on the drug problem but on which in-depth evidence is
scarce, including access to controlled medicines, international cooperation on drug
matters, alternative development in drug cultivation areas, and the nexus between
drugs and crime.
As in previous years, the World Drug Report 2020 is aimed at improving the
understanding of the world drug problem and contributing to fostering greater
international cooperation in order to counter its impact on health, governance and
security.
The accompanying statistical annex is published on the UNODC website:
wdr.unodc.org
Vienna International Centre, PO Box 500, 1400 Vienna, Austria
Tel: +(43) (1) 26060-0, Fax: +(43) (1) 26060-5866, www.unodc.org
6
OTHER DRUG POLICY ISSUES
2020
ISBN 978-92-1-148345-1
